左心低形成症候群(hypoplastic left heart syndrome: HLHS)の治療成績は向上しているが依然としてハイリスク疾患である.
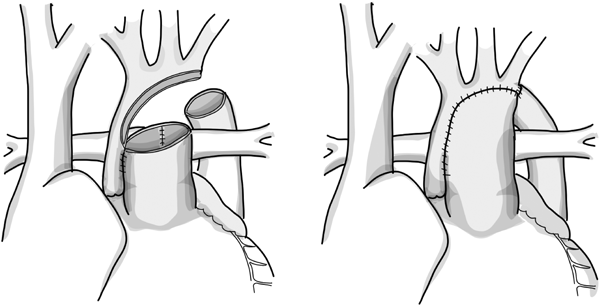
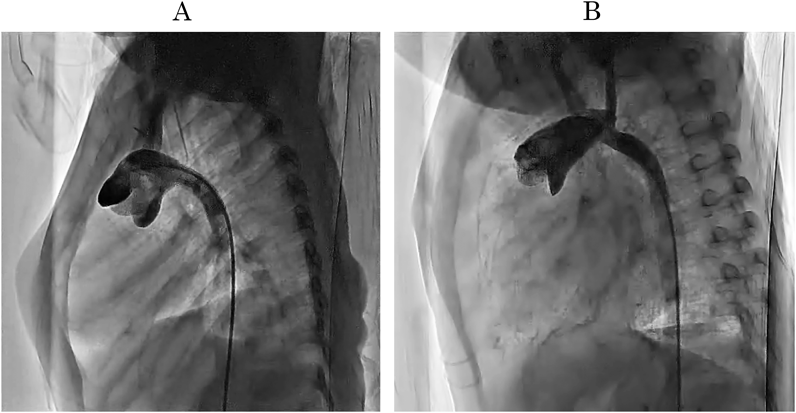
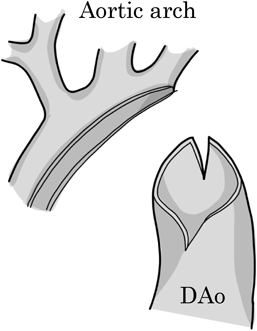
【大動脈再建】広い流路を確保する必要があり,大動脈の狭窄は後負荷増大とそれによる肺血流増加によって術後心不全の要因となる.広い流路のために組織補填を行うことが主流であるが本邦では自己組織を主体とした再建が多い.
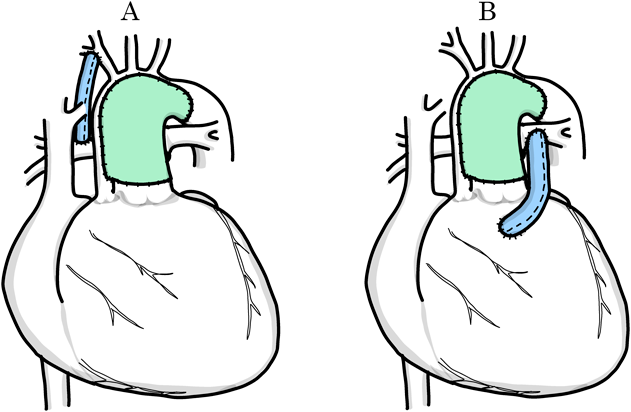
【肺動脈再建】肺血流量は適正である必要があり,肺血流過剰は心容量負荷となり血流不足は低酸素血症を生じる.右室–肺動脈導管の利点は血行動態の安定性にあり,心機能低下や三尖弁逆流のある術前状態の不良な症例では特に選択枝であると考えられる.一方で右室切開とそれに伴う心室機能障害,導管狭窄の懸念がある.
【両側肺動脈絞扼】本邦では多くの施設で初回姑息術として行われている.低体重,未熟児,脳出血合併,早期CPB手術の合併症を減らす点で効果があり,新生児期から乳児期に高度な開胸手術を延期することで神経発達を含む長期転帰で利益をもたらすことが期待される.
【体外循環】部分的脳灌流は本邦で広く行われており,超低体温完全循環停止下が主流である欧米でも近年増加している.下半身送血も本邦では広く行われているが,海外では標準的方法とはなっていない.下半身送血により腎障害の軽減とICU滞在時間の短縮が期待される.
Although treatment for hypoplastic left heart syndrome has improved, this condition is still considered high-risk.
[Aortic reconstruction] Aortic stenosis causes postoperative heart failure by increasing afterload and thus pulmonary blood flow. Patch augmentation of the entire arch is a common reconstruction technique for creating a large flow path. In Japan, however, reconstruction with primarily autologous tissue is common.
[Pulmonary artery reconstruction] The pulmonary blood flow must be adequate. Excessive pulmonary blood flow causes cardiac volume overload, while insufficient blood flow results in hypoxemia. A right ventricular-pulmonary artery conduit provides hemodynamic stability. This is considered an option, particularly for patients with a poor preoperative condition, such as low cardiac function or tricuspid valve regurgitation. However, there are concerns about the right ventricular incision, which can lead to ventricular dysfunction, and conduit stenosis.
[Bilateral pulmonary artery banding] Many Japanese institutions perform bilateral pulmonary artery banding as the first palliative procedure. It significantly reduces the risk of low birth weight, prematurity, cerebral hemorrhage, and complications of early cardiopulmonary bypass. It is expected to improve long-term outcomes, including neurodevelopment, by postponing open chest surgery during the neonatal period.
[Extracorporeal circulation] Partial cerebral perfusion is widely used in Japan. Complete circulatory arrest by hypothermia is most commonly used in North America and Europe, though the number of such procedures has grown in recent years. Lower body perfusion is also commonly used in Japan, but it has not become the standard method in other countries. Lower body blood perfusion is expected to reduce renal failure and shorten the intensive care unit stay.