右心不全の病態生理と機能評価
徳島大学病院小児科
受付日:2021年5月20日
受理日:2021年8月29日
発行日:2021年12月1日
小児循環器領域において右室機能解析を要する場面は多いが,正確な右室機能を測定評価することは簡単ではない.右心不全を呈する病態を分類すると,圧負荷,容量負荷,心筋障害の3つの機序が原因として挙げられるが,実際には様々な程度でこれらは混在することが多い.これらのうち右室機能障害の最も重要な原因は肺高血圧症であり,圧負荷に対する右室機能解析は同疾患の予後規定因子として評価が重要であるというだけではなく,右室機能障害を来す他疾患への応用と右室挙動の普遍的な解析のための基軸研究となり得る点で意義深い.
本総説では正常右室の構造・機能を解説したのち,右室機能障害の評価方法について説明する.右室機能障害は,右室全体の収縮機能の変化だけでなく,収縮様式,右室-肺動脈カップリング,同期性,心室間相互作用,拡張能などの障害も含んでいることを解説していく.
Key words: right heart failure; right ventricular function; pulmonary hypertension; echocardiography; right ventricular–arterial coupling
© 2021 特定非営利活動法人日本小児循環器学会
正常な循環動態の維持に右室は重要ではないという認識が長年にわたり存在していた1).この概念は複雑先天性心疾患において,肺循環側心室を完全に排除するフォンタン循環の成立でさらに検証されることとなった2).このため右室の重要性は軽視される時代が続き,Forgotten chamberとも言われた.このことは右室が左室に比較して複雑な構造と評価困難な生理学的特性を有しているために基礎・臨床研究が進まなかったことにも起因していると考えられる.近年,先天性心疾患術前術後例や肺高血圧症のみでなく,拡張型心筋症,左心不全症例の予後や運動耐容能を決定する上においても右室機能が重要な役割を果たしていることが報告されるようになり3),右室機能評価の重要性に関心が高まっている.
臨床家が異常な右室の挙動を呈する症例を診た場合,その一次的原因として想起される病態は,1)右室圧負荷,2)右室容量負荷,3)右室心筋障害の3つであり,いずれであるのかを判断することになる.このような原因分類は,病態生理の理解や解析には有用であるが,これらの要因はしばしば混在することを前提として評価しなければならない.例えば,ファロー四徴症心内修復術後症例は右室機能評価を要する代表的な症例群であるが,肺高血圧・肺動脈狭窄による圧負荷,肺動脈弁逆流・三尖弁逆流による容量負荷,手術操作や長期の低酸素・圧容量負荷による心筋障害が混在して存在する.1症例における右室機能を考察する場合にも,1病態に対する右室の挙動を研究する場合にも,これら3つの要因の間には密接な関係があり簡単に切り離すことはできないという認識が大切である.
右室機能障害の最も頻繁な原因は肺高血圧症であり,また右室機能は進行した肺高血圧症患者の臨床転帰を決定するに最も重要な要因である4–6)
.第1群に分類される肺動脈性肺高血圧症は年間100万人あたりの発症率が1~2例という稀な疾患であるにもかかわらず7),同疾患における右室機能評価の基礎研究・臨床研究が注目されているのは,予後因子として重要であるということだけではなく,右室機能障害の解析モデルとして臨床研究上の重要性があり,他疾患への応用と推察が可能である基軸研究となり得るためである.
本総説では正常右室の構造・機能を解説したのち,右室機能障害の評価方法について説明する.右室圧負荷は上記のごとく右室機能障害の3つの要因のうち最も頻度が高く,重要度が高い病態であるために重点を置いて述べる.そのなかで右室機能障害は,右室全体の収縮機能の変化だけでなく,収縮様式,同期性,心室間相互作用,拡張能などの障害も含んでいることを解説していく.
右室容積は左室より10~15%ほど大きく,自由壁は2~5 mmと薄く,心筋重量は左室の1/6~1/3ほどである8, 9).解剖学的に右室は流入路,肉柱部・心尖部,流出路・漏斗部に分けられる10).流出路の容積は正常例では右室拡張期容積の約20%を占める11).また,ヒトの右室の心筋細胞は左室心筋細胞に比べて約15%小さいことが知られている12).心筋細胞が小さいために,右室はコンプライアンスが高いにもかかわらず,膠原繊維は左室よりも約30%多い13).
左室心筋は3層構造(内斜走筋,輪状筋,外斜走筋)を形成するが,右室は2層から構成される.右室の表層(心外膜側層)は右室壁厚の25%を占め,主として房室溝に平行な円周方向(circumferential)の線維で形成されている14)(Fig. 1).一方,右室深層(心内膜下層)は縦方向優位(長軸,longitudinal)の心筋線維で構成され,心尖部から乳頭筋,三尖弁,右室流出路へ連続している.心内膜側であるため縦方向線維は早期に収縮を開始し,その量的優位性から,縦方向の短縮は右室収縮の多くを占めている15).
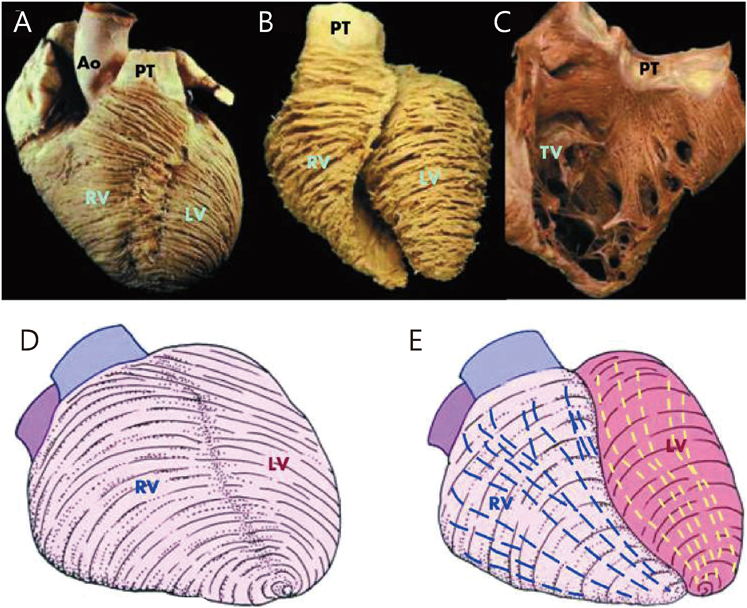
(A) A normal heart viewed from the front shows the circumferential to oblique arrangement of the myofibres in the subepicardium. (B) Myofibres lying deeper than the subepicardium retain the circumferential arrangement in the right ventricle but change from oblique to circumferential in the left ventricle. (C) The right ventricle is opened to show the longitudinally arranged subendocardial myofibres. The lower panels depict in simplistic fashion the subepicardial myofibres (D) and the deeper myofibres (E) in the ventricles of the normal heart. The superficial or subepicardial myofibres are arranged more or less circumferentially in a direction that parallel to the atrioventricular groove and encircle the subpulmonary infundibulum. The superficial fibres turn obliquely toward the cardiac apex to cross the interventricular groove and continue into the superficial myofibres of the left ventricle. The deep myofibres are longitudinally aligned, apex to base. Ao, aorta; LV, left ventricle; PT, pulmonary trunk; RV, right ventricle; TV, tricuspid valve. Figure modifies from Ho SY, et al. [ref. 14] with permission.
このような右室解剖と心筋線維の走行・構成から,右室の駆出様式は4つの異なる収縮パターンに分類される.(1)三尖弁が心尖部方向に牽引されることによる縦方向の短縮,(2)右室自由壁の横断方向(transverse)の短縮(ふいご様運動),(3)左室収縮により中隔の曲率半径が短縮して中隔が右室へ突出する運動,(4)心外膜側の円周方向の心筋線維が左右心室で共有されているため,自由壁が中隔を越えて牽引されることによる右室の前後方向の短縮である16).左室は右室の駆出に対しても重要な役割を果たしており,右室拍出量の20~40%を担っていると報告されている17, 18)
.これは主に中隔の収縮によるものだが,前述のような円周方向への牽引の寄与も大きい19, 20).
右室は高度な同期性と体系的な収縮様式を呈している.心尖部は流出路よりも20~50 msecほど早く収縮することで右室は蠕動運動のような動きをする8, 11, 21)
.漏斗部の収縮が遅いことは右室血流がスムーズに肺動脈へ駆出されることに貢献している.また,縦軸方向には流入路は流出路よりも収縮末期に及ぶ収縮を示し,水鉄砲様・ピストンポンプ様の収縮形態を示すと報告されている22).
渦形成が血流の方向転換と駆出の効率化に寄与している左室とは対照的に,右室腔内の血流パターンは比較的流線型であり,流入路から流出路まで滑らかな曲線を描く中隔に沿う経路をたどる23–25)
(Fig. 2).このような血流様式の相違は流入路と流出路が鋭角である左室とは対照的に右室形状が滑らかな曲線を呈するためである.また,低い右室圧は右室腔内の流れの方向転換を生じさせるという作用にとって合目的であると考えられる.右室心尖部の収縮・駆出率は他の部位に比較して小さいことが報告されている21, 26, 27)
.つまり,心尖部の役割は,駆出にあるのではなく,流入路から流出路へのスムーズで持続的な血流を維持させることであると考えられる21, 24)
.このような過程のなかで流出路において形成されるらせん状の流線は肺動脈への流れの安定性やエネルギーロスの最小化にも貢献している23).
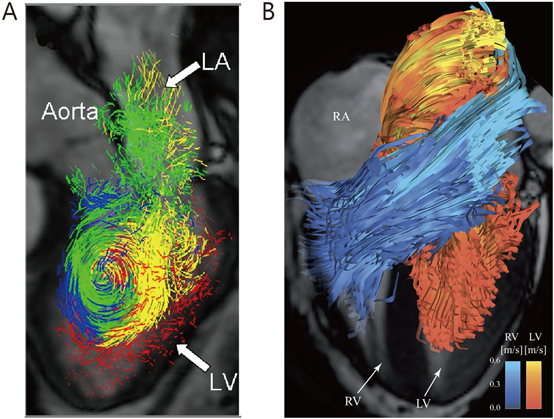
(A) LV direct flow at mid-diastolic phase. Vortex formation can be visualized. It is reported to contribute to the LV performance. (B) RV (blue) and LV (red) direct flow at early diastolic filling. The RV apex was more excluded from flow events than the apical region of LV. Direct flow in the RV moved from inflow to outflow with a gradual curvature around the infundibular septum compared with the more acute bend in the mid to apical ventricle observed in the LV. The RV geometry theoretically allows for an easy intraventricular transit of blood which does not require sustained vortex formation. LA, left atrium; LV, left ventricle; RV, right ventricle. Figure modifies from Fredriksson AG, et al. [ref. 24] and Eriksson J, et al. [ref. 25], with permission.
健常者では右室縦方向の短縮が右室の収縮機能の大部分を占めていると考えられる.これは心内膜側にある縦方向繊維が右室壁の約75%を占めていることからも推測される15, 28)
.そのために右室機能の指標として三尖弁輪収縮期移動距離(tricuspid annular plane systolic excursion; TAPSE),右室自由壁縦方向ストレイン(right ventricular longitudinal strain; RVLS),三尖弁輪収縮期最大移動速度(S′)など縦方向の心エコー図測定法が広く用いられている.最近の研究では,肺高血圧症においては右室の横断方向の動き,ふいご様運動が重要であり16, 29–31)
,縦方向の短縮よりも全体的な右室機能との相関性が高いとも報告されている29).これらの結果は肺高血圧が進行すると右室の駆出は縦方向ではなく,横断方向の壁運動に依存することを示している15, 28, 32)
.また,類似の病態では右室自由壁円周方向ストレイン(right ventricular circumferential strain; RVCS)のほうがRVLSよりも駆出を反映しているとの報告もあり,進行した重度の肺高血圧症では,右室縦方向の計測のみでは充分ではないことが示されている33).さらに右室自由壁縦方向の短縮は,心臓手術後の胸壁との癒着や心膜切開などによって影響を受け,術後の右室機能障害を正確に反映できなくなるため,右室内腔面積変化率(right ventricular fractional area change; RVFAC)や右室駆出率(right ventricular ejection fraction; RVEF)などの指標によって評価することも勧められている34).
右室機能評価の最も簡便で非侵襲的な検査方法は経胸壁心エコー検査である.心エコー検査による右心系の容量計測,右室収縮能および拡張能の評価は一般化しつつある35).Table 1およびFig. 3に米国心エコー図学会,欧州心臓病学会から提示されている成人の右心系評価の基準値を示す35, 36)
.人種間の相違,性別,年齢や体格による正常値の補正が必要であることは認識されているが,小児の正常値は各指標において充分に用意されているとは言えない37, 38)
.
| Variable | Abnormal |
|---|---|
| Chamber dimensions | |
| RV basal diameter | >41 mm |
| RV subcostal wall thickness | >5 mm |
| RVOT PSAX distal diameter | >2.7 cm |
| RVOT PLAX proximal diameter | >3.3 cm |
| RA major dimension | >5.3 cm |
| RA minor dimension | >4.4 cm |
| RA end-systolic area | >18 cm2 |
| Systolic function | |
| TAPSE | <17 mm |
| Tissue Doppler peak velocity (S′) at the annulus | <9.5 cm/s |
| Pulsed Doppler MPI | >0.40 |
| Tissue Doppler MPI | >0.54 |
| FAC | <35% |
| dP/dt (Doppler-derived) | <400 mmHg |
| EF (3D echocardiography) | <45% |
| RV free wall longitudinal strain | <20% |
| Diastolic function | |
| E/A ratio | <0.8 or >2.1 |
| E/E′ | >6 |
| Deceleration time | <120 msec |
| FAC, Fractional area change; MPI, myocardial performance index; PLAX, parasternal long-axis; PSAX, parasternal short-axis; RA, right atrium; RV, right ventricle; RVD, right ventricular diameter; RVOT, right ventricular outflow tract; TAPSE, tricuspid annular plane systolic excursion. Table modifies from Rudski LR, et al. [35], and Harjola VP, et al. [36] with permission. | |
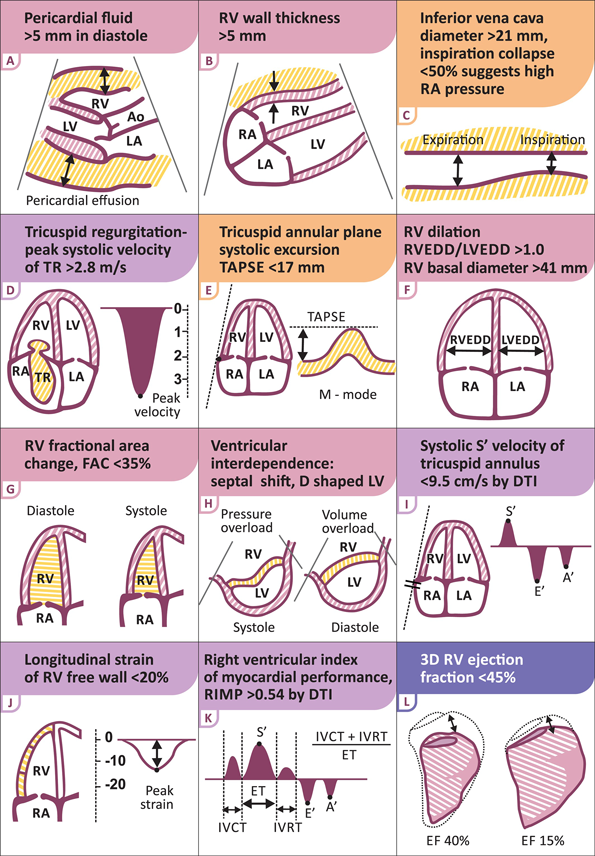
Ao, aorta; DTI, Doppler tissue imaging; EF, ejection fraction; ET, ejection time; FAC, fractional area change; IVC, inferior vena cava; IVCT, isovolumic contraction time; IVRT, isovolumic relaxation time; LA, left atrium; LV, left ventricle; LVEDD, left ventricular end-diastolic diameter; RA, right atrium; RIMP, right ventricular index of myocardial performance; RV, right ventricle; RVEDD, right ventricular end-diastolic diameter; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation. Figure modifies from Harjola VP, et al. [ref. 36] with permission.
RVFAC, TAPSEおよびS′などの記録は,右室に焦点を当てた心尖部四腔断面像(RV–focused apical 4-chamber view)で右室の最大径を示す画像を得るように心がけることが肝要である35).また,これらの指標は角度依存性であること,容量依存性であることに注意しなければならない.TAPSEは17 mm未満では異常所見とする.右室は複雑な構造を持つため通常の断層心エコー検査で駆出率を測定するのは困難である.その代替法として右室の拡張末期面積と収縮期面積から右室の収縮能を評価する方法がRVFACである.RVFAC<35%が異常所見とされる.右房圧は下大静脈径と呼吸性変動から推定する.下大静脈径21 mmを区切りとして50%以上の呼吸性変動の有無と合わせて評価する(Fig. 3).3D心エコー検査では右室容積とRVEFを直接定量化することができ,2D測定に関連する問題点を克服するとされている.3D検査で得られたRVEFは予後推測に関して優れていることが証明されてきており,最近では各ガイドラインにおいてもスペックルトラッキング法を用いたストレイン測定や3Dエコーを用いた指標による評価の推奨レベルが上ってきている.
右室は壁厚が薄く,容積と表面積の比率が低いため,コンプライアンスが高く,前負荷の増加には対応しやすいが,後負荷の急激な上昇には対応できない特徴がある.右室は肺高血圧などによって正常の約5倍の後負荷に直面する可能性があり,これは全身性高血圧や大動脈狭窄症のときに生じる正常の約1.5~2.0倍の後負荷増加よりもはるかに大きい(Fig. 4).後負荷増大時は左室のように求心性肥大による壁応力の軽減機序がうまく働かずにむしろ右室内腔は拡大し,容易にポンプ機能の破綻を来す.
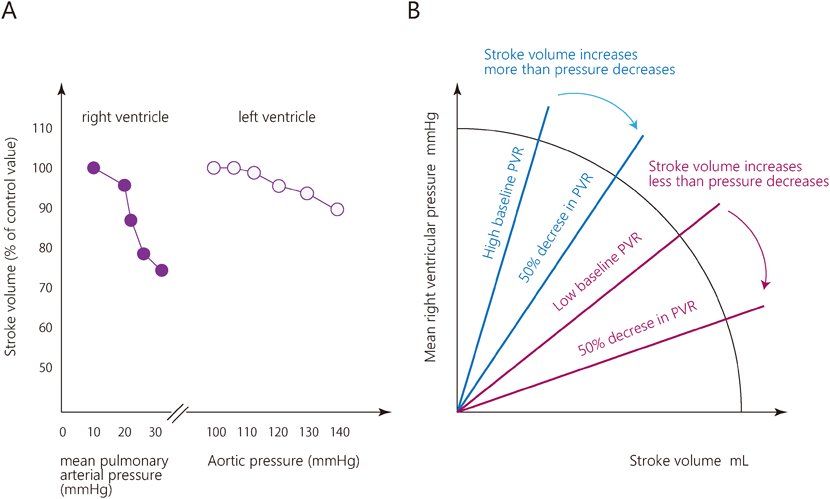
(A) Comparison of the effect of ejection pressure on ejection fraction in the RV and the LV. Note that for any incrementation ejection pressure, the decrement in ejection fraction is much greater in the RV than in the LV. (B) The pump function graph relates mean right ventricular pressure and stroke volume and can be obtained by changes in arterial load. The slopes of the straight lines are pulmonary vascular resistance (PVR). The relationship explains the effect of decreasing the arterial load on pressure and SV. When baseline PVR is high, a decrease in PVR mainly causes an increase in SV, while at lower baseline PVR the pressure is more affected. PVR, pulmonary vascular resistance. Figure creates from Haddad F, et al. [ref. 10] and Vonk Noordegraaf A, et al. [ref. 44].
肺高血圧症における右室機能不全は,右室が圧負荷の増加に適応できないときに起こる.圧負荷に対する心室の適応とは,心室充満圧を上昇させることなく,一回拍出量(SV)を維持するプロセスである39).右室は肺動脈圧負荷の増加に対して,Anrep効果などによる心筋収縮力の増大39–41)
,右室壁厚を増加(すなわち心室肥大)させて壁応力を減少させることによる適応(ラプラスの法則)40),神経性・体液性調節機構などにより順応する.この初期の強心反応はホメオメトリック適応と呼ばれる過程であり,心室は心筋の強心作用の増大で対応し41, 42),心室の形状を変えることなく1回心拍出量が回復する42).しかし,収縮能をこれ以上高めることができない場合には,後負荷の増加に対する唯一の効果的な反応として右室の拡張が残り,これはヘテロメトリック適応として知られるプロセスであり,右室の拡張末期容積の増加によって同程度の1回心拍出量が確保される39, 43)
.疾患が進行すると,右室のさらなる容積拡張は中隔の左室側への偏位を伴い,これが左室の収縮能と拡張期充満を低下させ,心拍出量を低下させる43).右室拡大が顕著となると三尖弁逆流の増加が惹起され,さらに右室拡大が引き起こされる.これらの病態とその代償として心室充満圧が上昇し,最終的には臨床的に非代償的段階へと進行していく18, 43, 44)
(Fig. 5).
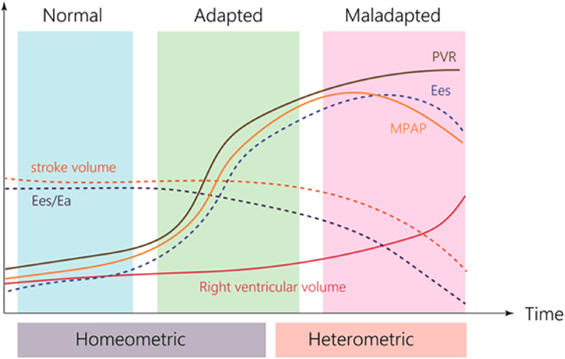
During the adapted homeometric phase, contractility increases to maintain the ratio Ees/Ea, but does so insufficiently, so that the Ees/Ea progressively declines along with an almost parallel decrease in stoke volume. Later in the process, RV volume increases, and Ea increases as a result of the increased heart rate and somewhat increasing PVR, whereas Ees decreases. heterometric adaptation (Starling’s law) is turned on. The ratio Ees/Ea is decreased, implying uncoupling of heart and load and a decrease in RV efficiency with rapid progressive increase in RVEDV and poor prognosis. PVR, pulmonary vascular resistance; MPAP, mean pulmonary arterial pressure. Figure modifies from Vonk Noordegraaf A, et al. [ref. 43] with permission.
右室,肺動脈それぞれの弾性腔としての特性を,右室収縮末期エラスタンス(Ees)と肺動脈エラスタンス(Ea)として定量化した場合の両者結合のバランスが右室—肺動脈カップリング(Ees/Ea)とされ,機能的駆出率,心拍出効率なども含めた右心系の循環動態を示す重要な因子である45)(Fig. 6).
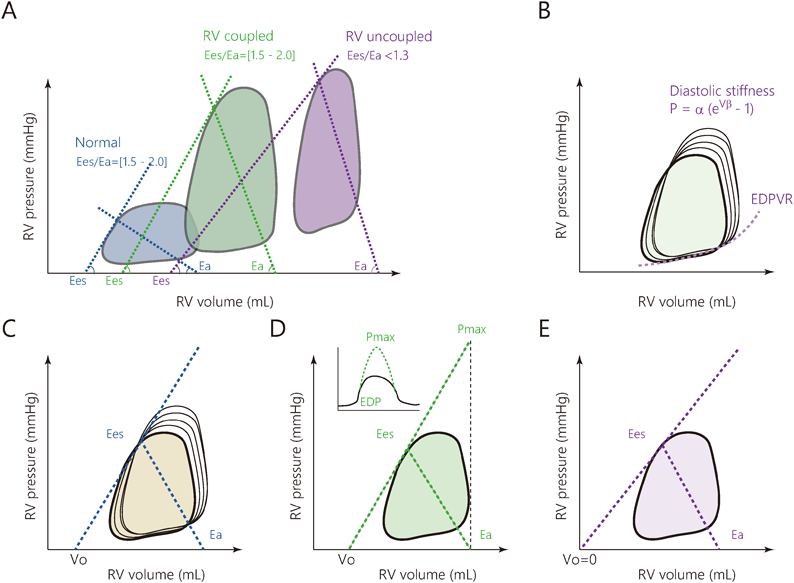
(A) Pressure-volume loop analysis and estimation of ventriculo-arterial coupling. (B) Information of load-independent RV diastology can be obtained by Pressure-volume loop analysis, with estimation of the diastolic stiffness constant β and end-diastolic elastance. The β coefficient is obtained by fitting a nonlinear exponential curve through the diastolic points at the beginning of diastole and end-diastole (end-diastolic pressure-volume relation, or EDPVR). (C) Methods for estimation of ventriculo-arterial coupling were shown. The multi-beat method requires obtaining different sets of pressure-volume loops at decreasing levels of preload. (D) In the single beat method, the RV pressure waveform tracing is used for estimation of Pmax. (E) In the volumetric method, V0 is assumed to be equal to zero, and Ees is estimated by the ratio of end-systolic pressure to end-systolic volume. EDP, end-diastolic pressure; EDPVR, end-diastolic pressure-volume relationship; RV, right ventricle. Figure creates from Vonk Noordegraaf A, et al. [ref. 43] and Bernardo RJ, et al. [ref. 45].
下大静脈の部分的閉塞46, 47)
,またはバルサルバ法48, 49)
によって前負荷を変化させながら心室圧容積関係を描くマルチビート法から得られた収縮期末圧容積関係(end-systolic pressure-volume relationship; ESPVR)は固有の心室収縮特性を示す.この傾きがEesである.ESP=Ees×(ESV−V0)の関係となる(ESP,収縮末期圧;ESV,収縮末期容積;V0,収縮期非伸展容積,ESPVRの容積軸切片).収縮末期のエラスタンスであるEesは一般的に最大エラスタンスの近似値として認められている8).最大エラスタンスは正常右室では収縮末期の少し前に起こるが,肺高血圧症例では収縮末期に起こる.これは右室圧負荷がかかった場合の圧容積関係が三角形ではなく,左室に類似した四角形になることからも推測される.Eaは右室収縮末期圧をSVで割った値(RVESP/SV)として得られる.
マルチビート法は技術的に複雑で日常的な臨床使用には適していない.そのため,簡略化したシングルビート法が提案されているが50, 51)
,この方法についても前提条件や制限を考慮する必要がある52).右室等容性収縮末期圧Pmaxの推定には1心拍の圧容積ループが必要であり,Ees=(Pmax-ESP)/SV, Ea=ESP/SVとして推定される.この方法の背景にある仮定は,Pmax-ESPの関係の線形性,および右室圧力波形トレースからのPmaxの決定であり,これは駆出を伴わない心室収縮(isovolumetric contraction)が正常な駆出拍動と同じESPVRを持つことを仮定している39).
安静時における正常な右室は,Ees/Ea>1の心筋代謝効率のよい状態で拍動している.最小のエネルギーコストで駆出するための最適なEes/Eaは正常右室で示されるように1.5から2.0であるとされている18, 30)
.肺高血圧による後負荷増大(Ea上昇)があるとEes/Eaは低下して1.0に近づく.さらに右室収縮が低下した状況(Ees低下)では,Ees/Eaは1.0以下に低下する.このように,Ees/Eaは循環系に起こる変化を高感度に反映することのできる循環指標であるといえる.
マルチビート法,シングルビート法よりもさらに簡略化された方法に容積法(volumetric method)がある.Ees=ESP/ESV, Ea=ESP/SVと近似される.Ees/Eaには共通項ESPがあり,Ees/Ea=SV/ESVと簡略化することができる53, 54)
.さらに,Ees/Ea=SV/ESV=(EDV−ESV)/ESVは1/(1/EF-1)に等しく,EFに規定されることにもなる.この方法の前提条件はESPVRのX軸の切片V0がゼロであることであるが,重度の肺高血圧や右心不全の場合にはこの前提は満たされない55).容積法の利点は,主に容積の推定に依存し,RV圧の侵襲的な測定を必要としないことである54).また,平均肺動脈圧(meanPAP)は,正常な右室収縮末期圧の妥当な近似値である.このため,Ea=meanPAP/SVとして計算できる.さらに,Ea=meanPAP/SV=TPR×SV×HR/SV=TPR×HRとなり,Eaは,全肺抵抗(TPR)に心拍数(HR)をかけたものとしても算出でき,肺血管抵抗(PVR)と心拍数の積も代替する近似値として提示される43, 56).他にも右室と肺動脈のカップリングEes/Eaを代替するいくつかの指標が提案されているが,これらは主に右室機能を負荷指標で除したものである.最も一般的な指標としては,TAPSEを収縮期肺動脈圧(sPAP)で割った比率57, 58)
,肺動脈脈圧を右心房圧で除した値(Pulmonary artery pulsatility index; PAPi)59),組織ドプラの収縮期波S′を体表面積で補正した右室収縮末期内腔面積(RV end-systolic area index; RVESAi)で割った比率などが利用されている60).これらの指標は単純な比率であるという利点があり,臨床的には有用であるが,右室機能および後負荷を生理学的論理性をもって代替している訳ではないことに注意する必要がある61–63)
.
心不全における右室収縮能障害のもう一つの大切な要素は,心室内,心室間,房室間での同期不全である.効率的な心拍出は2心室の収縮と弛緩が同期することによって得られる.右室内同期不全は,疾患の初期段階から存在し64),蠕動運動の喪失21),右室自由壁負荷および壁応力の不均一性の増悪をもたらし65),臨床像の悪化と関連している66).症状の進行は左室内の同期不全も惹起させることでさらに増悪する.右室機能障害が進行した段階では,右室収縮は顕著に延長し,肺動脈弁閉鎖を超えてしまうことがある(post-systolic isovolumic contraction).また,このような病態では,左室が既に弛緩している間にも右室は駆出を続ける心室間同期不全が顕著となる67–69)
(Fig. 7).その結果,心室中隔の左室側への偏位に伴う左室拡張能低下と左室充満不全,心拍出量低下につながる70).心臓は心膜という比較的伸展性に乏しい膜に囲まれた閉鎖腔内に存在することも右室拡大に伴う左室の圧排,狭小化を惹起して左室充満不全を来す.拡張期における心室間相互作用の悪化と右室コンプライアンスと弛緩能の低下を伴う右室拡張機能障害は心不全をさらに悪化させる71).
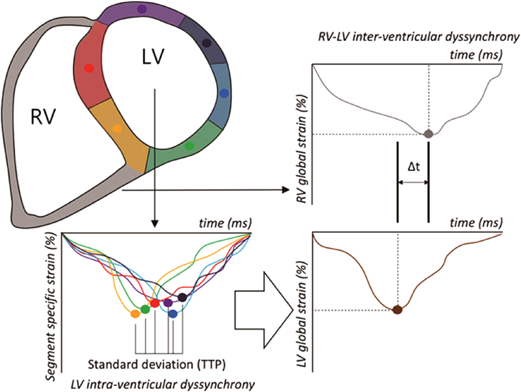
LV intraventricular dyssynchrony was analyzed by strain time-to-peak generated for 6 separate LV segments. RV–LV interventricular analysis was performed by comparing global LV and RV strain time to peak. LV, left ventricle; RV, right ventricle. Figure modifies from Schäfer M, et al. [ref. 69] with permission.
拡張能は心機能の重要な決定要因である.拡張期の充満は心筋の弛緩,収縮した心筋に蓄えられた弾性エネルギー・復元力,心室のスティッフネス(硬さ)および心房の収縮に依存する72).拡張能は上記のごとく異なる機序と時相から構成されているため,単一の独自指標で説明することはできない.右室拡張能を評価する指標には,(1)右房圧(RAP)および右室拡張末期圧(RVEDP),(2)右室充満プロファイル(心エコー検査におけるE波およびA波に基づく),(3)弛緩相指標(等容性拡張期(IVRT),dP/dt最小値,圧減衰の時定数τ),および(4)圧容積関係の解析によって特定される右室スティフネスなどの受動的特性がある10).
右房圧または右室拡張末期圧は,右心カテーテル検査時に直接測定するか,下大静脈径とその虚脱性を評価することにより非侵襲的に推定することができる35).また,右房圧の上昇は肝静脈,門脈,腎静脈のドプラ解析で確認することができる73).右室拡張機能障害の初期は弛緩障害を反映したE波低下によって特徴づけられ,拡張能障害後期は右室スティフネス上昇を反映したE/A比の増加が認められる.組織ドプラから得られた拡張早期波E′波を測定してE/E′が6以上になると,右室充満圧が上昇している判定基準となる73)(Table 1).しかし,実際にはファロー四徴症術後74, 75)
,肺高血圧症76),心不全症例76)において右室側E/E′が侵襲的検査から得られた拡張期充満圧を正確には反映しにくいことが示されている.左室拡張能指標としてのE/E′と比較すると,右室拡張能評価における有用性は落ちると言わざるを得ない.弛緩相指標のうち,等容性拡張期(IVRT)は三尖弁輪外側の組織ドプラ波形やパルスドプラ波形を用いて非侵襲的に測定できる.IVRTの増加は弛緩の障害と右房圧上昇を反映している77–79)
.しかし,この指標は心拍数と前負荷に大きく依存し,右房圧が顕著な異常高値を示すと偽正常化する可能性があるため,予後判定や臨床応用には限界がある80).等容性弛緩時定数(τ)は,肺高血圧症例では上昇していることが報告され,弛緩能のゴールドスタンダードとの意見もあるが81),右室圧は比較的低値となってから右室圧変化の最小値(dP/dt_min)を呈するために,左室と同様に本指標が有用であるか否かはさらなる検討を要するものと思われる71).拡張後期の拡張能であるスティッフネス評価の代表的な指標として,負荷を変えた拡張末期の点からなる曲線(end-diastolic pressure-volume relationship; EDPVR)を作成して,指数関数RVEDP=α(eVβ−1)に近似して求める係数(β)がある.RVEDVは右室拡張末期容積,αは係数,βがstiffness constantである.βは負荷非依存性のStiffness指標となるが,侵襲的にもその算出は難しい.そのため,心室最小圧から拡張末期にかけての圧変化を同期間の容積変化で除した傾きをchamber stiffness(K)として簡略化する試みもある82).今後,臨床的にも汎用される心室スティッフネスの指標の確立が望まれる.
右室は解剖学的にも病態生理学的にも左室とは異なる.左室の生理学的知識を直接右室に適用することはできない.右室機能は多くの心血管病変や循環器疾患の予後を決定する上で重要な役割を果たしていることが報告されている.各疾患に対する右室の挙動と臨床症状は,圧負荷,容積負荷,心筋障害の様々な組み合わせの結果である.負荷非依存性の右室収縮特性を示す指標の確立は望まれるが,現状では単純で簡便な評価方法を示すことは難しい.右室の解剖と病態生理と力学を理解することで,右室の収縮と充満の理解が深まる.将来,右心不全療法の治療の確立や診療ガイドラインが成立するためには,日常診療での右室機能評価の一般化が必要である.そのためには新たなモダリティの開発や簡便な測定方法,指標に関するさらなる研究が望まれる.
利益相反に関する事項はありません.
1) Kagan A: Dynamic responses of the right ventricle following extensive damage by cauterization. Circulation 1952; 5: 816–823
2) Fontan F, Baudet E: Surgical repair of tricuspid atresia. Thorax 1971; 26: 240–248
3) Meyer P, Filippatos GS, Ahmed MI, et al: Effects of right ventricular ejection fraction on outcomes in chronic systolic heart failure. Circulation 2010; 121: 252–258
4) Champion HC, Michelakis ED, Hassoun PM: Comprehensive invasive and noninvasive approach to the right ventricle-pulmonary circulation unit: State of the art and clinical and research implications. Circulation 2009; 120: 992–1007
5) Vanderpool RR, Saul M, Nouraie M, et al: Association between hemodynamic markers of pulmonary hypertension and outcomes in heart failure with preserved ejection fraction. JAMA Cardiol 2018; 3: 298–306
6) Vonk Noordegraaf A, Chin KM, Haddad F, et al: Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur Respir J 2019; 53: 1801900
7) Hoeper MM, Humbert M, Souza R, et al: A global view of pulmonary hypertension. Lancet Respir Med 2016; 4: 306–322
8) Dell’Italia LJ: The right ventricle: Anatomy, physiology, and clinical importance. Curr Probl Cardiol 1991; 16: 653–720
9) Kawel-Boehm N, Maceira A, Valsangiacomo-Buechel ER, et al: Normal values for cardiovascular magnetic resonance in adults and children. J Cardiovasc Magn Reson 2015; 17: 29
10) Haddad F, Hunt SA, Rosenthal DN, et al: Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation 2008; 117: 1436–1448
11) Geva T, Powell AJ, Crawford EC, et al: Evaluation of regional differences in right ventricular systolic function by acoustic quantification echocardiography and cine magnetic resonance imaging. Circulation 1998; 98: 339–345
12) Ashley LM: A determination of the diameters of ventricular myocardial fibers in man and other mammals. Am J Anat 1945; 77: 325–363
13) Weber KT: Cardiac interstitium in health and disease: The fibrillar collagen network. J Am Coll Cardiol 1989; 13: 1637–1652
14) Ho SY, Nihoyannopoulos P: Anatomy, echocardiography, and normal right ventricular dimensions. Heart 2006; 92 Suppl 1: i2–i13
15) Brown SB, Raina A, Katz D, et al: Longitudinal shortening accounts for the majority of right ventricula rcontraction and improves after pulmonary vasodilator therapy in normal subjects and patients with pulmonary arterial hypertension. Chest 2011; 140: 27–33
16) Kovács A, Lakatos B, Tokodi M, et al: Right ventricular mechanical pattern in health and disease: Beyond longitudinal shortening. Heart Fail Rev 2019; 24: 511–520
17) Konstam MA, Kiernan MS, Bernstein D, et al: Evaluation and management of right-sided heart failure: A scientific statement from the American Heart Association. Circulation 2018; 137: e578–e622
18) Lahm T, Douglas IS, Archer SL, et al: Assessment of right ventricular function in the research setting: Knowledge gaps and pathways forward. An official American Thoracic Society Research Statement. Am J Respir Crit Care Med 2018; 198: e15–e43
19) Naeije R, Badagliacca R: The overloaded right heart and ventricular interdependence. Cardiovasc Res 2017; 113: 1474–1485
20) van Wolferen SA, Marcus JT, Westerhof N, et al: Right coronary artery flow impairment in patients with pulmonary hypertension. Eur Heart J 2008; 29: 120–127
21) Calcutteea A, Chung R, Lindqvist P, et al: Differential right ventricular regional function and the effect of pulmonary hypertension: Three-dimensional echo study. Heart 2011; 97: 1004–1011
22) Hayabuchi Y, Ono A, Homma Y, et al: Temporal sequential pattern of right ventricular free wall contraction in normal children. Circ J 2017; 81: 1699–1706
23) Sengupta PP, Narula J: RV form and function: A piston pump, vortex impeller, or hydraulic ram? J Am Coll Cardiol Img 2013; 6: 636–639
24) Fredriksson AG, Zajac J, Eriksson J, et al: 4-D blood flow in the human right ventricle. Am J Physiol Heart Circ Physiol 2011; 301: H2344–H2350
25) Eriksson J, Carlhäll CJ, Dyverfeldt P, et al: Semi-automatic quantification of 4D left ventricular blood flow. J Cardiovasc Magn Reson 2010; 12: 9
26) Fernandez-Friera L, Garcia-Alvarez A, Guzman G, et al: Apical right ventricular dysfunction in patients with pulmonary hypertension demonstrated with magnetic resonance. Heart 2011; 97: 1250–1256
27) Vitarelli A, Mangieri E, Terzano C, et al: Three-dimensional echocardiography and 2D–3D speckle-tracking imaging in chronic pulmonary hypertension: Diagnostic accuracy in detecting hemodynamic signs of right ventricular (RV) failure. J Am Heart Assoc 2015; 4: e001584
28) Kind T, Marcus JT, Westerhof N, et al: Longitudinal and transverse movements of the right ventricle: Both are important in pulmonary arterial hypertension. Chest 2011; 140: 556–557
29) Kind T, Mauritz GJ, Marcus JT, et al: Peri-operative right ventricular dysfunction: The anesthesiologist’s view. Cardiovasc Diagn Ther 2020; 10: 1725–1734
30) Bosch L, Lam CSP, Gong L, et al: Right ventricular dysfunction in left-sided heart failure with preserved versus reduced ejection fraction. Eur J Heart Fail 2017; 19: 1664–1671
31) Gorter TM, van Veldhuisen DJ, Bauersachs J, et al: Right heart dysfunction and failure in heart failure with preserved ejection fraction: Mechanisms and management. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2018; 20: 16–37
32) Kind T, Mauritz GJ, Marcus JT, et al: Right ventricular ejection fraction is better reflected by transverse rather than longitudinal wall motion in pulmonary hypertension. J Cardiovasc Magn Reson 2010; 12: 35
33) Hayabuchi Y, Sakata M, Kagami S: Right ventricular myocardial deformation patterns in children with congenital heart disease associated with right ventricular pressure overload. Eur Heart J Cardiovasc Imaging 2015; 16: 890–899
34) Grønlykke L, Korshin A, Holmgaard F, et al: Severe loss of right ventricular longitudinal contraction occurs after cardiopulmonary bypass in patients with preserved right ventricular output. Int J Cardiovasc Imaging 2019; 35: 1661–1670
35) Rudski LG, Lai WW, Afilalo J, et al: Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 2010; 23: 685–713, quiz, 786–788
36) Harjola VP, Mebazaa A, Čelutkienė J, et al: Contemporary management of acute right ventricular failure: A statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. Eur J Heart Fail 2016; 18: 226–241
37) Bredy C, Soulatges C, Guillaumont S, et al: How should we determine normal echocardiographic right ventricle function reference values in pediatrics? Int J Cardiovasc Imaging 2019; 35: 259–226
38) Cantinotti M, Giordano R, Scalese M, et al: Nomograms for echocardiographic right ventricular sub-costal view dimensions in healthy Caucasian children: A new approach to measure the right ventricle. J Cardiol 2018; 71: 181–186
39) Bellofiore A, Chesler NC: Methods for measuring right ventricular function and hemodynamic coupling with the pulmonary vasculature. Ann Biomed Eng 2013; 41: 1384–1398
40) Wang Z, Chesler NC: Pulmonary vascular wall stiffness: An important contributor to the increased right ventricular afterload with pulmonary hypertension. Pulm Circ 2011; 1: 212–223
41) Naeije R, Brimioulle S, Dewachter L: Biomechanics of the right ventricle in health and disease (2013 Grover Conference series). Pulm Circ 2014; 4: 395–406
42) Cingolani HE, Perez NG, Cingolani OH, et al: The Anrep effect: 100 years later. Am J Physiol Heart Circ Physiol 2013; 304: H175–H182
43) Vonk Noordegraaf A, Westerhof BE, Westerhof N: The relationship between the right ventricle and its load in pulmonary hypertension. J Am Coll Cardiol 2017; 69: 236–243
44) Vonk-Noordegraaf A, Haddad F, Chin KM, et al: Right heart adaptation to pulmonary arterial hypertension: Physiology and pathobiology. J Am Coll Cardiol 2013; 62 Suppl: D22–D33
45) Bernardo RJ, Haddad F, Couture EJ, et al: Mechanics of right ventricular dysfunction in pulmonary arterial hypertension and heart failure with preserved ejection fraction. Cardiovasc Diagn Ther 2020; 10: 1580–1603
46) Tello K, Seeger W, Naeije R, et al: Right heart failure in pulmonary hypertension: Diagnosis and new perspectives on vascular and direct right ventricular treatment. Br J Pharmacol 2019; 178: 90–107
47) Boulate D, Mercier O, Guihaire J, et al: Pulmonary circulatory: Right ventricular uncoupling: New insights into pulmonary hypertension pathophysiology. Pulmonary Hypertension Cham. Springer International Publishing, 2016, pp. 241–253
48) Tedford RJ, Mudd JO, Girgis RE, et al: Right ventricular dysfunction in systemic sclerosis-associated pulmonary arterial hypertension. Circ Heart Fail 2013; 6: 953–963
49) Hsu S, Houston BA, Tampakakis E, et al: Right ventricular functional reserve in pulmonary arterial hypertension. Circulation 2016; 133: 2413–2422
50) Brimioulle S, Wauthy P, Ewalenko P, et al: Single-beat estimation of right ventricular end-systolic pressure-volume relationship. Am J Physiol Heart Circ Physiol 2003; 284: H1625–H1630
51) Westerhof N, Stergiopulos N, Noble MIM, et al: Cardiac power and ventriculo-arterial coupling. Snapshots of Hemodynamics Springer International Publishing, 2019, pp. 135–142
52) Philip JL, Chesler NC: Know your limitations: Assumptions in the single-beat method for estimating right ventricular-pulmonary vascular coupling. Am J Respir Crit Care Med 2018; 198: 707–709
53) Sanz J, Garcia-Alvarez A, Fernandez-Friera L, et al: Right ventriculo-arterial coupling in pulmonary hypertension: A magnetic resonance study. Heart 2012; 98: 238–243
54) Vanderpool RR, Rischard F, Naeije R, et al: Simple functional imaging of the right ventricle in pulmonary hypertension: Can right ventricular ejection fraction be improved? Int J Cardiol 2016; 223: 93–94
55) Trip P, Kind T, van de Veerdonk MC, et al: Accurate assessment of load-independent right ventricular systolic function in patients with pulmonary hypertension. J Heart Lung Transplant 2013; 32: 50–55
56) Pinsky MR: The right ventricle: Interaction with the pulmonary circulation. Crit Care 2016; 20: 266
57) Guazzi M, Bandera F, Pelissero G, et al: Tricuspid annular plane systolic excursion and pulmonary arterial systolic pressure relationship in heart failure: An index of right ventricular contractile function and prognosis. Am J Physiol Heart Circ Physiol 2013; 305: H1373–H1381
58) Tello K, Wan J, Dalmer A, et al: Validation of the tricuspid annular plane systolic excursion/systolic pulmonary artery pressure ratio for the assessment of right ventricular-arterial coupling in severe pulmonary hypertension. Circ Cardiovasc Imaging 2019; 12: e009047
59) Kochav SM, Flores RJ, Truby LK, et al: Prognostic impact of pulmonary artery pulsatility index (PAPi) in patients with advanced heart failure: Insights from the ESCAPE trial. J Card Fail 2018; 24: 453–459
60) Boulate D, Amsallem M, Kuznetsova T, et al: Echocardiographic evaluations of right ventriculo-arterial coupling in experimental and clinical pulmonary hypertension. Physiol Rep 2019; 7: e14322
61) Stevens GR, Garcia-Alvarez A, Sahni S, et al: RV dysfunction in pulmonary hypertension is independently related to pulmonary artery stiffness. JACC Cardiovasc Imaging 2012; 5: 378–387
62) Amsallem M, Boulate D, Aymami M, et al: Load adaptability in patients with pulmonary arterial hypertension. Am J Cardiol 2017; 120: 874–882
63) French S, Amsallem M, Ouazani N, et al: Non-invasive right ventricular load adaptability indices in patients with scleroderma-associated pulmonary arterial hypertension. Pulm Circ 2018; 8: 2045894018788268
64) Lamia B, Muir JF, Molano LC, et al: Altered synchrony of right ventricular contraction in borderline pulmonary hypertension. Int J Cardiovasc Imaging 2017; 33: 1331–1339
65) Walmsley J, van Everdingen W, Cramer MJ, et al: Combining computer modelling and cardiac imaging to understand right ventricular pump function. Cardiovasc Res 2017; 113: 1486–1498
66) Badagliacca R, Reali M, Poscia R, et al: Right intraventricular dyssynchrony in diopathic, heritable, and anorexigen-induced pulmonary arterial hypertension: Clinical impact and reversibility. J Am Coll Cardiol Img 2015; 8: 642–652
67) Burkett DA, Patel SS, Mertens L, et al: Relationship between left ventricular geometry and invasive hemodynamics in pediatric pulmonary hypertension. Circ Cardiovasc Imaging 2020; 13: e009825
68) Badagliacca R, Poscia R, Pezzuto B, et al: Right ventricular dyssynchrony in idiopathic pulmonary arterial hypertension: Determinants and impact on pump function. J Heart Lung Transplant 2015; 34: 381–389
69) Schäfer M, Collins KK, Browne LP, et al: Effect of electrical dyssynchrony on left and right ventricular mechanics in children with pulmonary arterial hypertension. J Heart Lung Transplant 2018; 37: 870–878
70) Marcus JT, Gan CT, Zwanenburg JJ, et al: Interventricular mechanical asynchrony in pulmonary arterial hypertension: Left-to-right delay in peak shortening is related to right ventricular overload and left ventricular underfilling. J Am Coll Cardiol 2008; 51: 750–757
71) Hayabuchi Y, Ono A, Homma Y, et al: Analysis of right ventricular myocardial stiffness and relaxation components in children and adolescents with pulmonary arterial hypertension. J Am Heart Assoc 2018; 7: e008670
72) Maksuti E, Carlsson M, Arheden H, et al: Hydraulic forces contribute to left ventricular diastolic filling. Sci Rep 2017; 7: 43505
73) Tang WH, Kitai T: Intrarenal venous flow: A window into the congestive kidney failure phenotype of heart failure? JACC Heart Fail 2016; 4: 683–686
74) Hayabuchi Y, Sakata M, Ohnishi T, et al: Ratio of early diastolic tricuspid inflow to tricuspid lateral annulus velocity reflects pulmonary regurgitation severity but not right ventricular diastolic function in children with repaired Tetralogy of Fallot. Pediatr Cardiol 2013; 34: 1112–1117
75) DiLorenzo M, Hwang WT, Goldmuntz E, et al: Diastolic dysfunction in tetralogy of Fallot: Comparison of echocardiography with catheterization. Echocardiography 2018; 35: 1641–1648
76) Fletcher AJ, Robinson S, Rana BS: Echocardiographic RV-E/e′ for predicting right atrial pressure: A review. Echo Res Pract 2020; 7: R11–R20
77) Yu CM, Sanderson JE, Chan S, et al: Right ventricular diastolic dysfunction in heart failure. Circulation 1996; 93: 1509–1514
78) Dambrauskaite V, Delcroix M, Claus P, et al: The evaluation of pulmonary hypertension using right ventricular myocardial isovolumic relaxation time. J Am Soc Echocardiogr 2005; 18: 1113–1120
79) Bréchot N, Gambotti L, Lafitte S, et al: Usefulness of right ventricular isovolumic relaxation time in predicting systolic pulmonary artery pressure. Eur J Echocardiogr 2008; 9: 547–554
80) Amsallem M, Boulate D, Kooreman Z, et al: Investigating the value of right heart echocardiographic metrics for detection of pulmonary hypertension in patients with advanced lung disease. Int J Cardiovasc Imaging 2017; 33: 825–835
81) Weiss JL, Frederiksen JW, Weisfeldt ML: Hemodynamic determinants of the time-course of fall in canine left ventricular pressure. J Clin Invest 1976; 58: 751–760
82) Masutani S, Little WC, Hasegawa H, et al: Restrictive left ventricular filling pattern does not result from increased left atrial pressure alone. Circulation 2008; 117: 1550–1554


This page was created on 2022-01-31T16:22:14.273+09:00
This page was last modified on 2022-03-08T10:43:34.000+09:00
このサイトは(株)国際文献社によって運用されています。