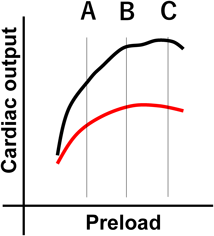
循環の基本となる心拍出量は1回拍出量と心拍数の積で表される.したがって,生理学の基本に立ち返り,1回拍出量が決まる機序を考える.Otto Frankはカエル摘出心を用いて「収縮直前の心筋長が大きければ収縮期に発生する最大圧が大きくなる」ことを見いだし,更にErnest H. Starlingは「心筋が収縮により発生するエネルギーenergy of contractionは,筋長に依存して決まり,生理的範囲内では,筋長が増えるにしたがい,発生エネルギーも増加する」という心臓法則を定義した.この法則を生体内の心臓に適応すると,心室内にある血液分だけ心筋は3次元方向に伸展し,およそ比例して1回仕事量の指標である“血圧×拍出量”を増やすことがわかる.Fig. 1は心臓法則を心臓全体に当てはめた,Frank–Starling曲線である.心収縮能が保たれている(black),そうでない(red)にかかわらず,血管特性が一定なら,前負荷増加(A→B)に伴い拍出量は増加する.
一方,輸液過剰のために循環不全に至った症例をしばしば紹介される.Frank–Starling曲線の説明でしばしば省略されがちであるが,Fig. 1に示すように,容量負荷が一定量を超えると心拍出量は増加しない(C).つまりこの曲線は,“心臓は容量負荷に伴って,ある範囲では心拍出量が増え,血圧も上昇する”,しかし“過剰になるとそれ以上増えない”,という情報を提供している.
したがって心臓法則のみに基づく管理は,容量負荷をはじめとする循環への介入によって“改善しない状況が近づいた”,あるいは“有効ではない”ことを経験等に基づいて感知し,治療介入を調整する管理が原則となる.たとえば,容量負荷(前負荷)に対する心臓の限界を推定する方法として,肺動脈楔入圧や左房圧,中心静脈圧を用いたForester分類やNohria–Stevenson分類が考案されているが,Forester分類は小児には侵襲性の高い指標であり,Nohria–Stevenson分類は周辺環境に影響を受けやすい小さい体格の症例において,客観性に乏しいことが問題である.
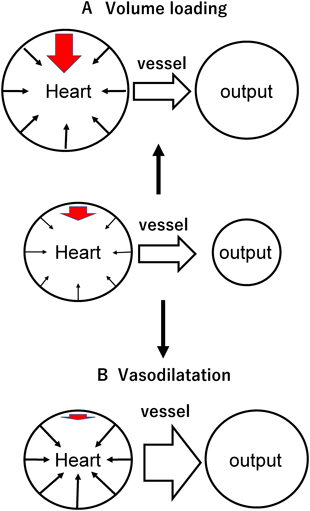
上記のような問題点を踏まえ,心室圧容積関係の概念と利点を概説する1).まず心臓法則を片隅において,心臓と臓器を血管が結ぶ単純なアナロジーをイメージする(Fig. 2).①血管特性が不変と仮定すると,心臓容積の増加に伴って心拍出量が増加し,血圧も心室内圧も上昇する(Fig. 2A: 容量負荷).これは心収縮力が低下した心臓でも同様だが,心拍出量および血圧上昇は緩やかとなる(Fig. 1).②心収縮性が一定かつ心容積も一定の場合に血管拡張が起きると血圧は低下し心拍出量は増加する(Fig. 2B: 血管拡張).反対に血管が収縮すれば血圧は上昇し,心拍出量は低下する.このことは1回拍出量と血圧が心臓特性(収縮性=縮むときに出せる力・拡張性=血液がどのくらい入れられるか),前負荷(与えられた心室容積),後負荷(血管収縮度)に規定される特徴があることを示す.
それでは心収縮が低下した症例(収縮不全心)に対して血管収縮薬・拡張薬を使用すると心拍出量と血圧の変化は正常心と比較してどのような反応示すだろうか?以下の選択肢から適切と思われるものを選んで以下を読み進めていただきたい.
- 選択肢:
- 正常心と比較し,血管収縮に伴う血圧上昇は小さく,血管拡張に伴う血圧低下は大きい
- 正常心と比較し,血管収縮に伴う血圧上昇は大きく,血管拡張に伴う血圧低下も大きい
- 正常心と比較し,血管収縮に伴う血圧上昇は小さく,血管拡張に伴う血圧低下も小さい
- 正常心と比較し,血管収縮に伴う血圧上昇は大きく,血管拡張に伴う血圧低下も大きい
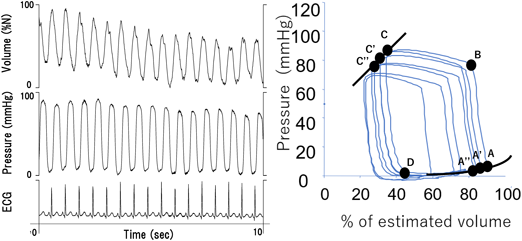
臨床でしばしば遭遇するこの問いには心室圧容積関係の概念を理解すると容易に答えることができる1, 2).まず心室圧と容積を同時に測定し(Fig. 3 left),心室圧を縦軸に,容積を横軸にとって心室周期を描いてみると平面上に1回拍出量と血圧(心室圧)の変動を示すループができる(Fig. 3 right,拡張末期A→B→収縮末期C→D).心室圧・容積を同時に計測した定常状態から,たとえば下大静脈を閉塞して心室容積を短時間に減少させ,連続したループを描いてみる(Fig. 3 left)と,それぞれのループは瞬時に容積(前負荷)が主に変化したもの(Fig. 3 right)であり,各時相において収縮性・拡張性で定義される心臓の特性が変化するには充分に短い,すなわち心臓特性はほぼ不変と考えられる.ここで各ループの左肩(C→C′→C″)の点を結んだ線は直線を示し,固有の心室収縮特性を示す収縮期末圧容積関係と呼ばれる(Fig. 4: a solid line,収縮末期圧:ESP=Ees×(ESV−V0)).心収縮性の高い心臓では傾き(Ees)が急峻(Fig. 4: a dotted line),低い心臓では緩慢となり,負荷条件に影響を受けにくい収縮性指標(Fig. 4a: end-systolic pressure-volume relationship, ESPVR)であることが明らかとなっている.また右下の点を結んだ線は指数関数(Fig. 3 right, A→A′→A″,拡張末期圧:EDP=α×eβ×EDV)に近似することができ,拡張末期圧が上がりやすい拡張能の低下した心臓は急峻に,拡張末期圧が上がりにくい柔らかい心臓は平坦に近づき,負荷条件に影響を受けにくい拡張性の指標(Fig. 4a: end-diastolic pressure-volume relationship, EDPVR)である.では心臓に対する前負荷および後負荷はこの平面で表すことができるだろうか? 全身に一定の血液を送り出すのに要する血圧を血管特性であると定義すれば,図示された直線の傾き=実効動脈エラスタンス(Fig. 4b, effective arterial elastance: Ea=収縮末期圧/1回拍出量)で後負荷としての血管特性を表現することができる.EaのX軸との交点=ループの最も右側の心室容積が拡張末期容積=心室前負荷である.したがって,循環を規定する要素のうち心拍数以外のもの,拡張末期心室容積(前負荷),体血管特性(後負荷)をFig. 4bに,心臓収縮・拡張特性をFig. 4aに,つまり同じXY平面上に表現することができ,これらを統合して考えることが可能となる.
次に心収縮が低下した状態,すなわち緩やかな傾きの収縮期末圧容積関係を想定してみる(Fig. 5 right).Fig. 5 leftに心拍出量と血圧,後負荷Eaが同じであるが,心収縮に低下がない症例を示す.血管を拡張させる,すなわちEaの傾きを緩やかすると(Fig. 5: blue dotted line),収縮末期の圧・容積点(交点)は左下に移動し,両者とも血圧は低下し,心拍出量は増加することがわかる.収縮性の良い症例(Fig. 5 left)と比較して収縮性の低下している症例(Fig. 5 right)では血圧が低下しにくく,心拍出量はより増加する.逆に後負荷を増加させる(red dotted line)と収縮末期圧・容積点は右上に移動し,血圧は上昇しにくい一方で,心拍出量は著明に減少する.したがって設問の正答はcとなる.つまり,心収縮能の低下した症例では血管収縮・拡張に伴う心拍出量の変動が大きい.したがって収縮性の低下した心臓では,後負荷を低下させる治療の有用性が極めて高く,後負荷増強が心臓にとって強大な負荷となることもわかる.心室圧容積関係を考慮すると,血圧だけでなく心拍出量の変動も推定できることに是非注目してほしい.
Forester分類やNohria–Stevenson分類に基づいて判断されてきた循環に対する介入はしばしば判定が困難であり,臨床的有用性には疑問があった.循環管理における心室圧容積関係の導入は,循環が非常に論理的で議論が可能なものであることを明確に示した.下記に一例を提示する.
症例1
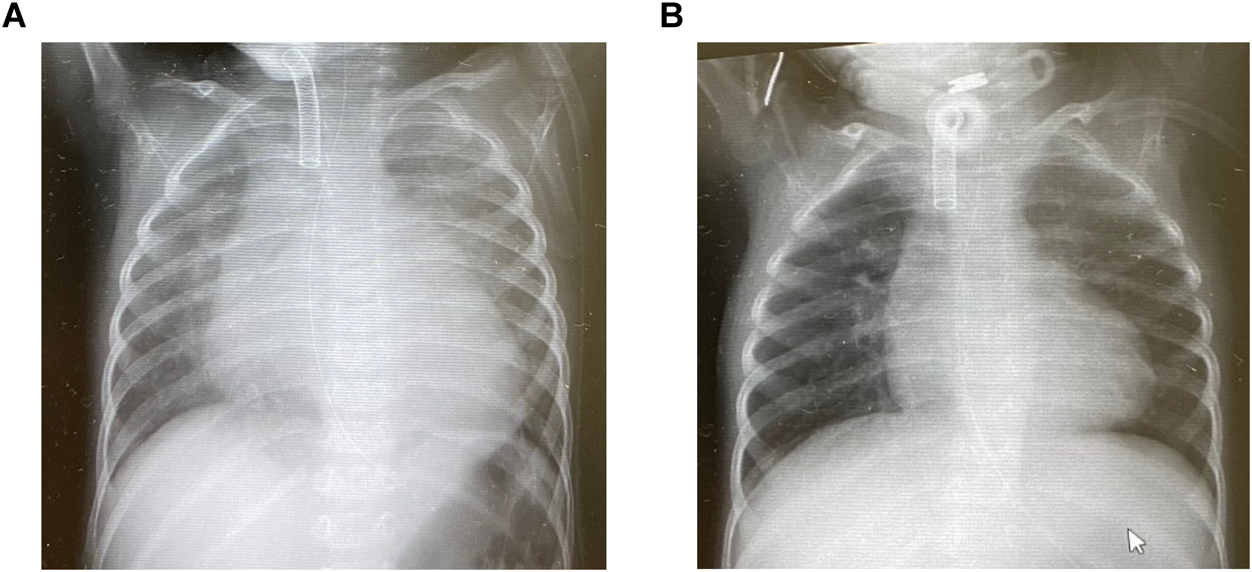
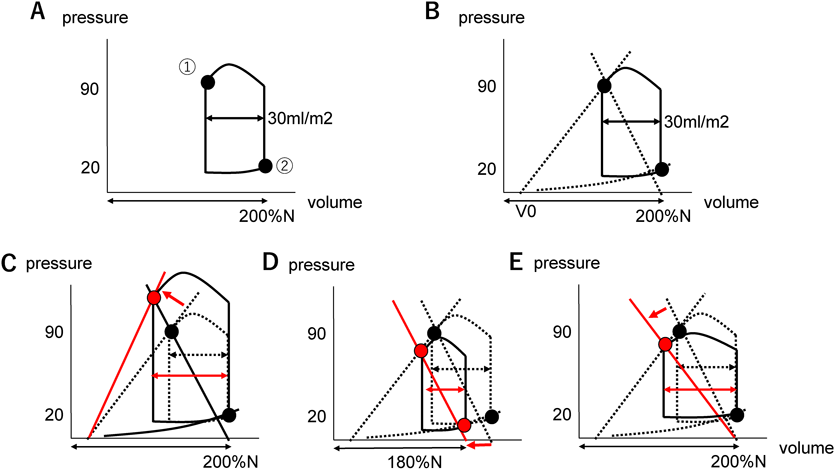
心筋緻密化障害の2歳男児.心収縮性の低下により,うっ血性心不全に至った症例である.末梢血中ナトリウム利尿ペプチドは上昇(7,879 pg/mL)し,胸部レントゲン写真では心拡大と肺うっ血像を認めた(Fig. 6A).心拍数は130/分,末梢血圧は90/40 mmHg,超音波検査では左室拡張末期径35 mm(正常値の135%),容積換算でおよそ正常値の200%,駆出分画(Simpson)30%であった.フロセミド/アルダクトン2 mg/kg/day,マレイン酸エナラプリル0.2 mg/kg/day,カルベジロール0.4 mg/kg/dayを内服していたが,心拡大進行し,管理を検討することとなった.
まず,縦軸に血圧,横軸に心室容積を取るグラフを作成する(Fig. 7A).上記の情報からおよその収縮末期圧容積点を記載する.肺うっ血像があり,僧帽弁閉鎖不全の血流速度が最大でも4m/sec程度と低下していることから左室拡張末期圧は低くないことが想定される(推定左房圧=90−4*42=90−64=26 mmHg, Fig. 7B拡張末期圧容積点).超音波検査から1回拍出係数が30 mL/m2(左室流出路断面積×velocity–time integral),駆出率が30%と推定されるため,左室拡張末期容積は100 mL/m2(拡張末期容積係数=1回拍出係数/駆出率=30 mL/m2/0.30),実効動脈エラスタンスは大まかに推定できる(Ea=収縮末期圧/1回拍出係数)3).これらをグラフに記載するとFig. 7Bとなり,想定される仮想心室圧容積関係を点線で記載する(便宜的に心室圧が0 mmHgに近似されるときの心室容積:V0=0 mLとしてもよいし,概算しても良い4–6)).
次に,循環変化を推定・考察する.心収縮性を改善できれば1回拍出量は増加し,血圧も上昇する(Fig. 7C).しかし,本疾患が慢性心不全を発症した心筋症であることを考慮すると,循環作動薬で著明な改善は得られない可能性が高いことも想像に難くない.容量負荷を行えば心拍出量は増加するが,拡張末期容積増加に伴う拡張末期圧上昇をきたし,肺うっ血はいくらか増悪する(Fig. 7D).血管拡張薬を用いると血圧低下の代償に心拍出量は増加する(Fig. 7E).特に収縮期末圧容積関係が急峻でない(心収縮能が低下している)本例では1回拍出量増加に比した血圧低下は大きくないはずである.利尿薬で容量負荷を軽減できれば心拍出量の低下は無視できないが,肺うっ血の軽減が期待できる(Fig. 7D).これらを念頭に置き,少量の容量負荷や血管拡張薬でどのような変化を示すかを考え,観察し,実際の心室圧容積関係を更に細かく推定・確定していく作業を行っていくと,詳細な循環管理が可能となる.
本症例では高度心不全治療への移行を希望されず,自宅で安寧に過ごすことが第一目標であった.呼吸状態が改善すれば希望が叶えられると判断し,拡張末期圧を極力下げることに主眼を置いて,脱水徴候に注意しながら水分制限を行った.水分制限に伴う血圧・心拍出量の低下は少しでも心室収縮性を改善させて補うことができればと考え,昨今のエビデンスに基づいて,少量ジゴキシンとピモベンダン0.1 mg/kg/dayを開始した.
これらによって,全身状態が改善し,在宅管理が可能となった.次の段階として,心筋のリバース・リモデリングが見込めないかと考えた.心筋酸素消費はESPVR, EDPVRおよび心室圧容積ループで囲まれた面積に正相関する7)ことが知られている.心筋収縮改善に伴い,心筋酸素消費は増加に転じるため,ヘモグロビン値12 g/dLを下限として輸血をためらわないこと,拡張末期圧上昇は冠血流増悪に関わることから体重を連日自宅で測定する水分管理を導入した.幸運なことに約半年の経過でリバース・リモデリングを導入することができ,BNPは11 pg/mLまで低下した.この症例では,心拡大は改善したが,依然少量の水分負荷で浮腫増悪をきたすことから,感染症・貧血に注意しつつ脱水気味のバランスで慎重に管理を継続している(Fig. 6B).
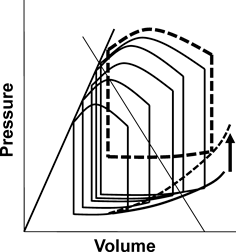
Fig. 1に示されるように,心不全が代償されていれば,前負荷動員によって心拍出量を増やすことができる.しかし非代償性心不全に至るとFrank–Starling機序は破綻を始め,前負荷に見合った拍出量増加が期待できず,更に前負荷を動員する生理反応が起き続ける(利尿低下・口渇増強等)悪循環に至る.この背景には心筋エネルギー効率の悪化,Laplaceの法則に基づく収縮性の低下,冠血流不全など様々な影響がある.このようなFrank–Starling機序の破綻には収縮不全に起因する容量負荷動員・過剰の病態だけでなく,基本病態としての心室拡張機能障害の存在も鑑別である(Fig. 8).一般に,心室拡張末期容積は静脈還流増加に伴って増加するが,心室容積が大きい状態(グラフの右方)では,拡張期末圧容積関係が急峻になり,心房還流圧上昇が心室拡張末期容積(前負荷)増加に寄与しにくい.結果として,心室の手前,すなわち心房や肺のうっ血増強が顕著となる.一方,拡張機能障害は正常以下,あるいはやや多い心室容積において,拡張期末圧容積関係が急峻となる病態を主に示す.心室拡張機能障害の診断は時に困難であるが,容量負荷に呼応した心室拡張末期容積(前負荷)増加が得られず,うっ血症状を呈する際に疑う8).そのメカニズムには心筋線維化に加え,慢性炎症等による微小血管障害,微細な虚血性変化が関わっていると考えられているが,不明な点も多い8–10).小児においても拡張機能障害は時に認められ11),ファロー四徴症や大動脈縮窄症などの術後症例に頻度が高い.開心術後の症例では収縮性心膜炎等の物理的な拡張障害も鑑別にあがる12).
肺循環側心室を欠くフォンタン循環では,循環血液量を増加させても,筋肉ポンプや静脈機能が還流を維持できず,心室拡張末期容積拡大に寄与できないことがある.すなわち,肺循環が律速段階となって,あたかも拡張機能障害に類似した病態を元来保持する循環であるが13),後に述べるように,本当に心室拡張機能障害が併存することも珍しくない.
このように,循環不全の症例に対する容量負荷では,拡張期心室圧容積関係を常に想定し,心室前負荷増加の程度と拡張末期圧・容積がどのような関係にあるかを想像する習慣をつけたい.発展的な内容であるが,心室圧容積関係を考慮しても有効な管理が提案できない場合,以下に示すような介入があることを合わせて紹介する.
先天性心疾患の循環管理でしばしば問題となるのがフォンタン循環である.フォンタン循環は肺循環と体循環を直列につないだ循環系を一つの心室で回す特異な循環であり,2心室循環と比較し,前述のように前負荷が増加しにくいこと,後負荷上昇に起因する低心拍出量をきたしやすいことの2点が特徴である2, 14).この循環特性に加え,生後早期からのチアノーゼや圧負荷,右心バイパス後の高いレニン-アンジオテンシン系活性13, 15),相対的に低いナトリウム利尿ペプチドの影響を受け,更に心血管系硬化をきたす悪循環を形成する13).そして遠隔期に至ると“静脈うっ血”によるうっ血性末梢臓器障害を背景に,血管抵抗が低下を始めることが推定されている6, 16).その結果,フォンタン術後早期から形成された硬い心血管系に対して,遠隔期の血管抵抗低下に伴う容量負荷需要がフォンタン不全発症に寄与する可能性が示唆されている6, 16–19).フォンタン不全の予防における血行動態管理の重要性が近年指摘されており19),フォンタン術後早期からフォンタン関連臓器障害が発症する前段階において,前負荷予備能低下の管理が極めて重要である20).
症例2
1歳4か月,フォンタン術後左心低形成症候群の男児である.この症例は開窓型フォンタン手術を行ったが,術後1日目には開窓が閉鎖した.術後2か月で蛋白漏出性胃腸症を発症し,CVPを下げる目的で強制的に体重を15%ほど減少させるドライサイド管理を行って緩解に導入した後,心臓カテーテル検査を施行した.腹部圧迫中の心室・下大静脈圧同時測定を示す(Fig. 9).軽い腹部圧迫によって拡張末期圧は20 mmHg付近から容易に中心静脈圧に近接した.すなわちドライサイド管理中の心室においてもわずかな容量負荷で拡張期末圧容積関係の急峻な心室容積域(容積変化あたりの心室圧上昇が大きい)に入る,硬い心臓が示唆された.この所見から,開窓が早期に閉鎖した原因は,周術期の水分負荷・3rdコンパートメントからの血管内回帰等によって左房–下大静脈圧較差低減が生じたと考えられた20).この知見に基づき,早期に再開窓手術を行い,合併した肺動脈狭窄の解除とともに容量負荷を最小限にした管理を行ったところ,開窓閉鎖をきたすことなく管理ができた.従来開窓の自然閉鎖は良好な循環を背景に起こると考えられてきたが,我々の検討では循環指標が必ずしも良好でない症例も多く自然閉鎖しており20),そのメカニズムを示唆する重要な症例である.
このように拡張機能障害が示唆された際には,拡張期心室圧容積関係を想定し,主心室が対処できる範囲の血管内容積・循環血液量で循環を維持する方法を模索することにより,フォンタン不全の予防に寄与できる可能性がある.また,下記のように刺激伝導系に対して介入することで機能的に容量負荷が可能となる症例もある.
症例3
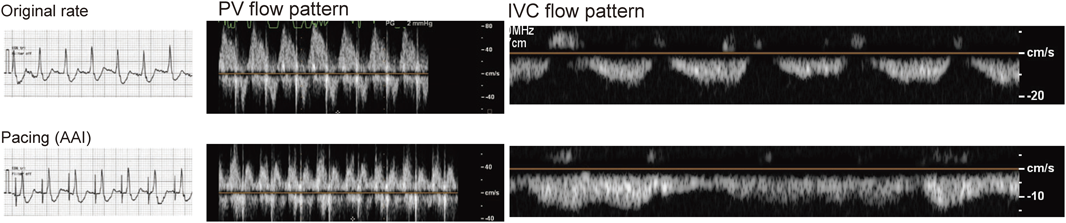
無脾症候群,単心房・単心室に対して開窓型フォンタン手術を施行した,術後2週間の1歳男児.いったん集中治療室に帰室したが,術後に発症した高度房室弁閉鎖不全に対して緊急体外式膜型人工肺(ECMO)管理を行い,1週間後に房室弁形成術を施行してECMO管理を離脱した.その後,中心静脈圧20~25 mmHgから1週間以上低下せず,浮腫の管理が困難で集中治療室を退室できなかった症例である.開窓はECMO前から確認できなかった.一酸化窒素吸入療法に加えシルデナフィル2 mg/kg/day,マシテンタン0.4 mg/kg/dayを使用したが,利尿に伴い血圧低下が著しく,セレキシパグ導入を開始したが経過は安定しなかった.心拍数は120~140 bpm,血圧は90/50 mmHgとほぼ変動ないが,利尿の都度,容量負荷を要した.利尿・容量負荷に伴う血圧の乱高下,胸部レントゲン写真の小さい心臓(CTR40%前後),全身性浮腫を伴う高中心静脈圧,駆出分画65%を超える良好な収縮機能は心室拡張機能障害を示唆した.一時的心房ペーシングによって心拍数を10~20/分増加しても,血圧・中心静脈圧とも変化は認めなかった.心電図では接合部調律か,上室性調律か判断が困難であった.当科コンサルトに際し,心収縮は非常に良好であったが,超音波検査時に心房・心室収縮タイミングが近接して見えたため,超音波検査で確認しながら一時的心房ペーシングを行った.やはり血圧・中心静脈圧ともペーシングによる変化は認めなかったが,心房・心室収縮のタイミングが乖離し,下大静脈波形・肺静脈波形とも改善を認めた(Fig. 10)ため,ペーシング下に循環管理を継続する方針とした.心筋肥厚や拡張末期容積に変化はなかったが,利尿に伴う血圧低下は軽減した一方,ペーシングを中止すると容量負荷依存性が再燃したため,恒久的ペースメーカーの適応と判断した.退室後1か月で心臓カテーテル検査を行ったところ,ペーシング可能な最低心拍数と自己調律との間に著明な循環指標の変化を認め,前負荷確保に心房ペーシングが有効であることが確認された(Table 1).面白いことに術後1年の検査ではペーシングによる循環のメリットは完全に消失し,循環不全に際して需要が高まることが確認された.本症例はフォンタン手術前に想定したとおり,中心静脈圧10 mmHg前後で心拍出係数3.0 L/min/m2以上が確保できる良好な循環が維持できていた.
Table 1 Hemodynamic response against atrial pacing | PMR 130 bpm | PMR 100 bpm | SR 95 bpm |
|---|
| CI (Fick), L/min/m2 | 3.00 | 2.74 | 2.20 |
| LVp, mmHg | 77/EDP 6 | 80/EDP 8 | 72/EDP 8 |
| PA wedge, mmHg | 4 | 6 | 7 |
| CVP, mmHg | 7–8 | 8 | 10 |
| SvO2, % | | 55 | 45 |
| CI: Cardiac Index, CVP: central venous pressure, LVp: Left ventricular pressure, PA: pulmonary artery, PMR: pacemaker rhythm, SR: sinus rhythm, SvO2: central venous pressure in central vein. |