先天性心疾患における心肺運動負荷テストの活用Cardiopulmonary Exercise Testing in Congenital Heart Disease
東京大学小児科Department of Pediatrics, The University of Tokyo ◇ Tokyo, Japan
発行日:2020年3月1日Published: March 1, 2020
運動耐容能低下は慢性心不全の主要症状の一つである.心肺運動負荷テスト(CPX)では,運動中の気道におけるガス交換を計測することで,心血管および換気システムの運動ストレスに対する反応を同時に調べることができる.運動中は,筋肉で消費・産生される酸素・二酸化炭素と,肺における外呼吸が心血管系を通じてカップリングしている.そのため,肺における外呼吸を調べることで,運動中の細胞呼吸の需要増加に対する心臓血管系の適応能力を明らかにすることができる.先天性心疾患(CHD)患者は,幼少期より心疾患とともに育ち,自分の生活スタイルを心疾患に適応させて暮らしているため,運動耐容能の低下があっても気づかないことが多い.そのため,CHD患者では,いわゆる“無症状”な場合でも,CPXにより客観的な評価を行い,潜在的な運動耐容能の低下を早期に検出することが重要である.また,運動耐容能低下の程度およびCPXによって得られるその他の指標は,CHDの患者において強い生命予後予測因子であることが示されている.CHDの患者は,外科手術やカテーテル治療などリスクの高い治療が必要になることがあり,Risk-stratificationの一つの手段として,精度の高い予後予測を行うことのできるCPXの果たす役割は大きい.この総説ではCHDにおけるCPXの結果の解釈および活用の仕方について概説する.
Exercise intolerance is one of the major symptoms of chronic heart failure. Cardiopulmonary exercise testing (CPX) allows for the simultaneous study of responses to cardiovascular and ventilator systems to a known exercise stress through the measurement of gas exchange at the airway. During exercise, oxygen consumption and carbon dioxide production at the contracting muscle are coupled with the external respiration at the lung through the cardiovascular system. Therefore, by studying external respiration in response to exercise, it is possible to address the functional competence of the cardiovascular system to meet the increased cellular respiratory demands during exercise. Objective assessment of exercise intolerance by means of CPX is especially important in patients with congenital heart disease (CHD), as they have made lifelong adaptations to their cardiovascular disease and its slow progression. Thus, they are not aware of the true extent of their exercise intolerance. Moreover, recent studies have demonstrated the ability of several CPX parameters to predict the long-term survival of patients with CHD. Because CHD patients often require high-risk surgical or catheter interventions and risk stratification based on individual risks is essential in this population, CPX plays a major role in the management of CHD. On the other hand, there are several pitfalls in interpreting the results of CPX in CHD. This review provides an overview of the interpretation and application of CPX in CHD.
Key words: cardiopulmonary exercise testing; congenital heart disease; prognosis; risk stratification; survival
© 2020 特定非営利活動法人日本小児循環器学会© 2020 Japanese Society of Pediatric Cardiology and Cardiac Surgery
運動耐容能低下は心不全の主要症状の一つであるため,これを正確に評価し,診断・治療に役立てることが,循環器疾患の患者の診療において重要である.運動中は,筋肉で消費・産生される酸素・二酸化炭素と肺における呼吸が心血管系を通じてカップリングしている.心肺運動負荷テスト(CPX)では,運動中の気道におけるガス交換を計測することで,末梢組織におけるエネルギー代謝や心肺機能とのカップリングを調べる.特に最大酸素摂取量(Peak VO2)は心血管・肺が末梢組織に酸素を供給する能力を反映し,総合的な心肺機能や運動耐容能の指標となる.自転車エルゴメータにおいて計測される仕事率(Work rate)は,運動の強度を表すが,筋肉で消費されるエネルギーを直接的に反映しないため,客観的な運動耐容能の指標としては不十分である.
心肺運動負荷検査の施行は,6歳頃より施行が可能である.自転車エルゴメータを用いる場合は,負荷装置のサイズの点から身長が125 cm以上であることが望ましい1, 2).先天性心疾患を有する患者に使用する場合は,主に,運動耐容能の客観的評価,運動耐容能低下の原因鑑別,予後予測などに用いられる.まず,運動耐容能は心不全の重症度の客観的指標となり,反復評価を行うことで薬物治療・手術・心臓リハビリテーションなどの介入の効果判定を行うことが可能である.先天性心疾患(CHD)患者では,幼少期より心疾患とともに育ち,自分の生活スタイルを心疾患に適応させて暮らしているため,運動耐容能の低下があっても気づかないことが多い.そのため,CHD患者では,いわゆる“無症状”な場合でも,CPXにより客観的な評価を行い,潜在的な運動耐容能の低下を早期に検出する事も重要である.また,多くの合併疾患を持ちうるCHDの患者において,運動耐容能の低下が必ずしも心血管系の異常に起因するとは限らず,CPXは運動耐容能低下の原因がどこにあるかの鑑別にも役立つため,主観的に運動耐容能の低下がある患者においても有用である.心血管系とそれ以外の理由による運動耐容能低下の鑑別に有用なパラメーターをTable 1に提示する3).近年,運動耐容能低下の程度およびCPXによって得られるその他の指標は,CHDの患者において強い予後予測因子であることが示されている4–7).また,Fontanなどのいくつかの疾患では,単回の評価だけでなく反復評価に基づく時系列変化も予後予測に有用との報告がある8, 9).CHDの患者は,外科手術やカテーテル治療などリスクの高い治療が必要になることがあり,Risk-stratificationの一つの手段として,精度の高い予後予測を行うことのできるCPXの果たす役割は大きい.
| Causes | Markers of abnormality |
| Obesity | Upward displacement of VO2-WR relationship |
| Lung diseases | Abnormal lung function test, low BR |
| Peripheral arterial diseases | Low ⊿VO2/⊿WR, Low ⊿VCO2/⊿WR, leg pain, exercise-induced hypertension |
| Psychological problems | Unique breathing pattern |
| Poor effort | Increased HRR, increased BR, peak RER<1.0, normal VT |
| VO2; oxygen consumption, WR; work rate, BR; breathing reserve, HRR; heart rate reserve, RER; respiratory exchange ratio, VT; ventilatory threshold | |
一般に運動負荷検査では,入院を要する合併症が0.05%以下,死亡が0.005%で起こるとされ10),これらのリスクについて十分に説明した上で検査を開始する.また,呼吸器疾患の有無がCPXの結果の解釈に影響するため,呼吸機能検査(肺活量と1秒率)を施行しておくことが望ましい.運動負荷にはトレッドミルを用いる方法と自転車エルゴメータを用いる方法と主に2種類あるが,それぞれ長所短所があり施設の好みにより選ばれていることが多い.運動強度の指標であるWork rateと酸素摂取量(VO2)の変化の比は予後予測に有用とされるが,自転車エルゴメータでの負荷ではWork rateを正確に定量化することができる.一方で,自転車エルゴメータの負荷では大腿四頭筋の疲労のためトレッドミルに比べて,Peak VO2が10%程度低く計測される3, 11).通常,CPXでは症候限界までの漸増運動を負荷するが,運動開始から8~12分で最大負荷に達するように,予測される心肺機能に応じて,負荷漸増の割合を決定する10).負荷中は,心電図,心拍数,血圧,呼吸数,酸素飽和度などのモニターに加え,被験者の状態をよく観察することが重要である.
Peak VO2は1分間に体重1 kgあたり取り込むことができる酸素の量(mL/kg/分)として表され,運動耐容能の客観的な指標として用いられることが多い.最大酸素摂取量は心拍出量,動脈血酸素含有量,運動している筋肉への血流の分配,筋肉の酸素取り込み能力などによって規定される.年齢や性別によって正常値が異なるため,年齢・体格からの予測値の何%という形で表記することもある.チアノーゼ性心疾患では,運動中の動脈血酸素含有量が低下などの様々な要因によりPeak VO2の低下を認める.Peak VO2は,先天性心疾患を含めた多くの心疾患において強い予後予測能力があることが示されているが,努力依存的(effort-dependent)なパラメーターであるために,十分な負荷がかかっていない場合は過小評価してしまう4).この数値によって運動耐容能評価や予後予測を行う際には,十分な運動努力がされたのかについて総合的に判断した上で数値を解釈することが重要である.成人先天性心疾患患者における,単変量としてのPeak VO2と5年生存率の関係をFig. 1に示すが,Peak VO2は正常値の下限である80%以下になると低ければ低いほど予後不良である7).一般的にpeak VO2 <14 mL/kg/分,または予測値の50%未満が予後不良とされ心臓移植の適応条件として採用されている.
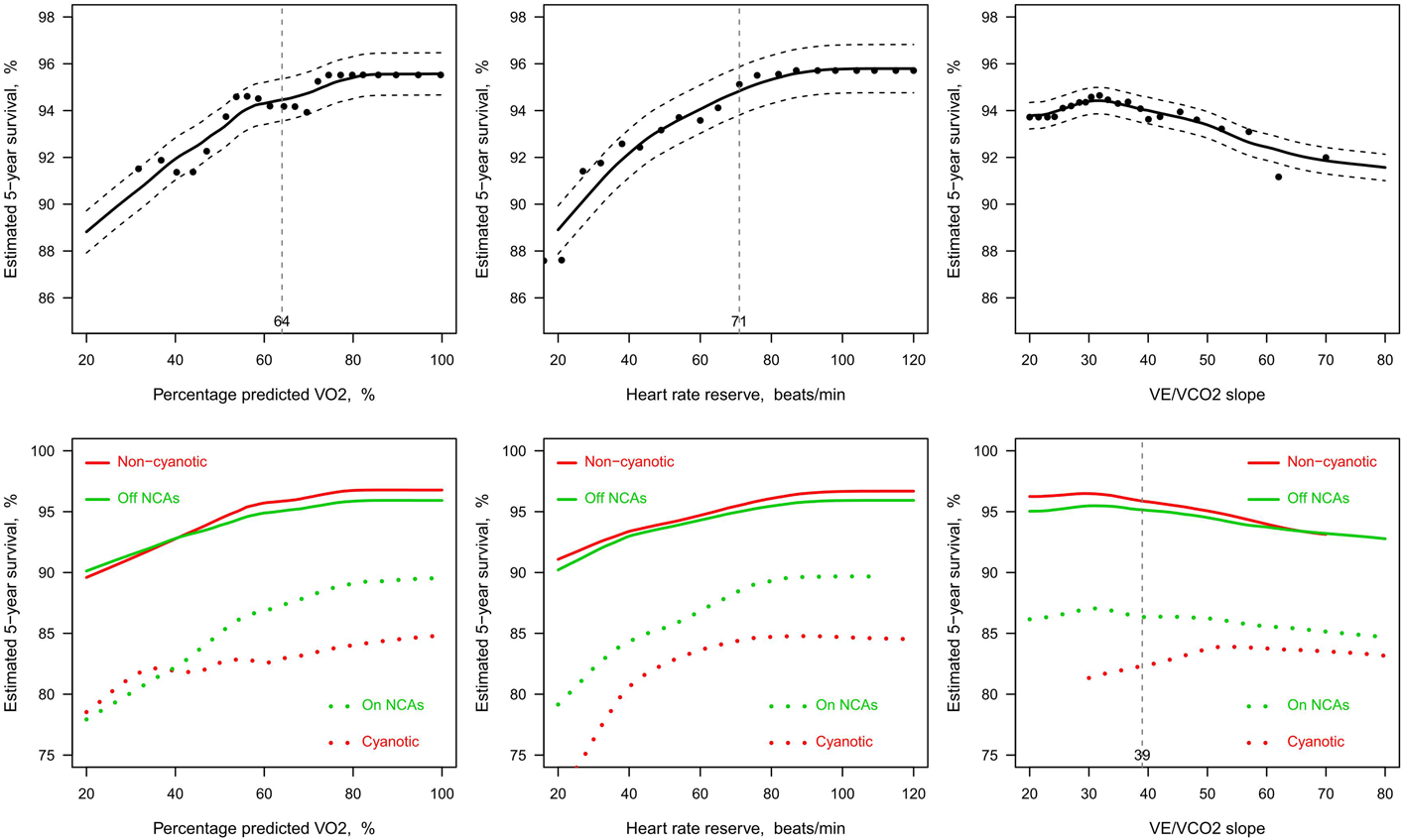
(Upper panels) The dots illustrate estimated 5-year survival as a function of (left panel) peak oxygen uptake (VO2), (middle panel) heart rate reserve and (right panel) VE/VCO2 slope for the whole population. The vertical dotted line shows cut-off values obtained by time-dependent ROC analysis. (Lower panels) Survival functions for non-cyanotic patients (red solid lines), cyanotic patients (red dotted lines), patients off negative chronotropic agents (NCA) (green solid lines) and patients on NCA (green dotted lines). The vertical dotted line for VE/VCO2 slope reflects the cut-off value for non-cyanotic patients as obtained by time-dependent ROC analysis. Reproduced from Figure 3 of reference 7).
運動の強さを増していくとき,筋肉のエネルギー消費に必要な酸素供給が追いつかなくなると,エネルギー産生における嫌気性解糖への依存度が高まり,最終代謝産物として乳酸がより多く産生され始める10).その結果,重炭酸イオンが乳酸の緩衝のために消費されるため,運動中の呼気に含まれる二酸化炭素が増加する.この呼気の様子を観察することにより決定したポイントを換気性作業閾値(VT)と呼ぶ.VTにはV-slope法や換気当量法などの様々な決定方法があるが,酸素摂取量の増加に比して換気量が過剰(相加的)に増加し始める運動強度での酸素摂取量と定義される.VTはFig. 2に示すように換気当量法やV-slope法を用いて,総合的に決定する.VTは通常,Peak VO2の45~65%程度となる.VTも運動耐容能の指標であり,さらに運動努力に依存しない安定したパラメーターではあるが,先天性心疾患においてはPeak VO2に比べて予後予測能力が劣ることが知られており,後に述べる運動処方の際の指標として使用することが多い7).

(1) Ventilatory equivalent method: In the time trend of the ventilatory equivalent for O2 (VE/VO2) and the ventilatory equivalent for CO2 (VE/VCO2), ventilatory threshold (VT, red line) is determined as the point at which VE/VO2 (purple open circles) systematically increases without an increase in VE/VCO2 (green triangles). This normally coincides with systematic increase in respiratory exchange ratio (yellow marks). (2) V-slope method: Plotting VCO2 as a function of VO2 for a progressively increasing work rate test (V-slope plot), after the first minute or so of increasing work rate, yields a progression of points that are linear with a slope of 1.0 (45 degree) or slightly less. The curve then breaks, with VCO2 increasing faster than VO2 so that the slope is now clearly above 1.0. The break point (red cross) where the slopes coincide is the ventilatory threshold. Figure was provided by Minato Medical Science
酸素摂取量に対する二酸化炭素排出量の比を呼吸交換比(RER)と呼ぶが,強い運動強度では,重炭酸イオンが乳酸の緩衝のために消費された結果として,運動中の呼気に含まれる二酸化炭素が増加し,RERの増加を認める.運動中のRERの最大値は運動努力の最も良い指標になると考えられている10).一般にpeak RER 1.1~1.15以上が達成された場合は,十分な運動努力がされたことを示すが,逆にpeak RERが1.0未満の場合は負荷が不十分であった可能性が高い.運動努力が十分であったかどうかについて,予測最大心拍数の85%が達成されたかどうかを指標にする場合もあるが,心不全患者においてはChronotropic incompetenceなどの心拍数が上昇しない病態が存在する場合やβ遮断薬を内服している場合などがあり,心拍数が運動努力の指標になりにくい.
換気量−二酸化炭素排出量関係の傾きは,VE/VCO2 slopeと呼ばれ換気の効率を表す.VE/VCO2 slopeが高いということは,換気をする割に二酸化炭素の排出ができていないことから,いわゆる“息切れ”の指標となる.心不全患者,特に肺うっ血を有する患者では,肺コンプライアンス低下に伴う死腔換気の増加により,好気的運動においても換気効率が低下している.VE/VCO2 slopeは好気的運動時に測定でき,運動努力に依存しない安定したパラメーターであることから心不全患者において高い予後予測能力を有することが知られている.ただし,右左シャントに伴う換気血流不均衡が存在するチアノーゼ性心疾患では,肺うっ血がなくても換気効率が低下しているためVE/VCO2 slopeが高くなり,予後予測には使用できない.非チアノーゼ性先天性心疾患においては,VE/VCO2 slopeが38以上で予後不良に関連すると報告されている6).
運動に見合った心拍数の調節が適切にできない現象つまり予測最大心拍数の85%が達成できない状態をChronotropic incompetenceと呼ぶが,Chronotropic incompetenceは慢性心不全の患者における予後不良因子として注目されている.運動中に心拍数をどのくらい増加させることができるか,つまり最大心拍数−安静時心拍数をHeart rate reserveと呼び,これはChronotropic incompetenceの指標となる.先天性心疾患において,Heart rate reserveはチアノーゼの患者でも安定して計測することができる予後予測能の高い指標である5).Fig. 1に示すようにHeart rate reserveの値自体はベータ遮断薬などの影響を受けるが,β遮断薬を内服している患者でも内服していない患者でも予後予測に有用であることが示されている7).Heart rate reserveはPeak VO2と同様に低いほど予後不良だが,特にHeart rate reserve ≦51 bpmで予後不良との関係が示されている5).
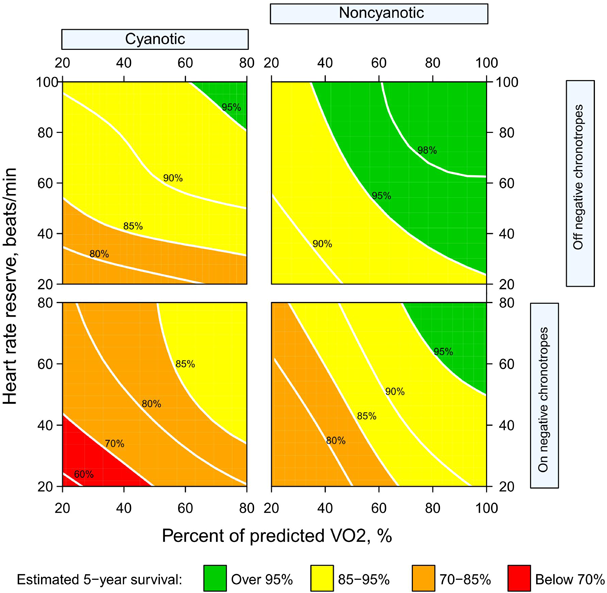
上で説明したCPX指標の特徴をTable 2にまとめる.一般にCPXでは十分な負荷がかかっていることが必要だが,CHDの患者では,日頃の運動不足により筋肉の疲労が生じやすく,十分な負荷をかけることができないことがあるため,Peak RERが1.10~1.15以上あるかどうかを参考に負荷が十分であったかどうかを判定する.Peak VO2やHeart rate reserveなどは負荷依存性が高いため,Submaximalな負荷では過小評価となる.一方で,VTやVE/VCO2 slopeなどの指標はSubmaximalな負荷のもとで行われた検査でも安定して計測することができる.しかし上述のようにVE/VCO2 slopeは,右左シャントの影響を受け,チアノーゼのある患者の予後予測には役立たない.このようにCHD患者においては,それぞれのCPXパラメーターが,運動負荷の程度,チアノーゼの有無,β遮断薬の内服の有無などの影響を受けるため,これらを総合して結果を解釈する必要がある.CPXパラメーターを用いた5年生存率の予測の一例を示す(Fig. 3)7).
| Effort-dependence | Influence of cyanosis | Influence of β blockers | |
|---|---|---|---|
| Peak oxygen consumption (VO2) | ++ | + | + |
| Ventilatory threshold(VT) | + | + | − |
| VE/VCO2 slope | − | ++ | − |
| Heart rate reserve | ++ | − | ++ |
Reproduced from Figure 5 of reference 7)
先天性心疾患の患者において,適度な運動を定期的に行うことは,最大酸素摂取量を増加させることが知られており,運動耐容能の低下がある患者でも身体的活動を行うことが推奨される12).心機能低下の程度,心室圧・容量負荷の程度,肺高血圧の有無,大動脈拡張の有無,運動誘発性不整脈の有無,失神の既往,運動中の低酸素血症の有無,抗凝固療法の有無,植え込み型デバイスの有無などの運動に関連するリスクを総合して,運動の種類や強度を決定する13, 14).この際,CPXを用い患者の運動に伴うリスクを明らかにしておくと同時に運動耐容能を客観的に評価しておくことが望ましい.通常慢性期の運動としては嫌気性代謝閾値レベル,最大酸素摂取量の40~60%,最高心拍数の40~60%程度の負荷が推奨されている15).
開示すべきCO I関係にある企業などはありません.
1) Paridon SM, Alpert BS, Boas SR, et al: American Heart Association Council on Cardiovascular Disease in the Young, Committee on Atherosclerosis, Hypertension, and Obesity in Youth: Clinical stress testing in the pediatric age group: A statement from the American Heart Association Council on Cardiovascular Disease in the Young, Committee on Atherosclerosis, Hypertension, and Obesity in Youth. Circulation 2006; 113: 1905–1920
2) Takken T, Bongers BC, van Brussel M, et al: Cardiopulmonary exercise testing in pediatrics. Ann Am Thorac Soc 2017; 14 Supplement_1: S123–S128
3) Wasserman K, Hansen JE, Sue D, et al: Principles of Exercise Testing and Interpretation. Lippincott Williams & Wilkins, 2005
4) Diller GP, Dimopoulos K, Okonko D, et al: Exercise intolerance in adult congenital heart disease: Comparative severity, correlates, and prognostic implication. Circulation 2005; 112: 828–835
5) Diller GP, Dimopoulos K, Okonko D, et al: Heart rate response during exercise predicts survival in adults with congenital heart disease. J Am Coll Cardiol 2006; 48: 1250–1256
6) Dimopoulos K, Okonko DO, Diller GP, et al: Abnormal ventilatory response to exercise in adults with congenital heart disease relates to cyanosis and predicts survival. Circulation 2006; 113: 2796–2802
7) Inuzuka R, Diller GP, Borgia F, et al: Comprehensive use of cardiopulmonary exercise testing identifies adults with congenital heart disease at increased mortality risk in the medium term. Circulation 2012; 125: 250–259
8) Cunningham JW, Nathan AS, Rhodes J, et al: Decline in peak oxygen consumption over time predicts death or transplantation in adults with a Fontan circulation. Am Heart J 2017; 189: 184–192
9) Cohen-Solal A, Choussat R, Chachques JC, et al: Serial assessment of cardiopulmonary exercise capacity after cardiomyoplasty for either ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol 1996; 77: 623–627
10) Balady GJ, Arena R, Sietsema K, et al; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology; Council on Epidemiology and Prevention; Council on Peripheral Vascular Disease; Interdisciplinary Council on Quality of Care and Outcomes Research: Clinician’s Guide to cardiopulmonary exercise testing in adults: A scientific statement from the American Heart Association. Circulation 2010; 122: 191–225
11) 大内秀雄:運動負荷試験.日小児循環器会誌2014; 30: 635–645
12) Longmuir PE, Brothers JA, de Ferranti SD, et al; American Heart Association Atherosclerosis, Hypertension and Obesity in Youth Committee of the Council on Cardiovascular Disease in the Young: Promotion of physical activity for children and adults with congenital heart disease: A scientific statement from the American Heart Association. Circulation 2013; 127: 2147–2159
13) Budts W, Börjesson M, Chessa M, et al: Physical activity in adolescents and adults with congenital heart defects: Individualized exercise prescription. Eur Heart J 2013; 34: 3669–3674
14) Fletcher GF, Ades PA, Kligfield P, et al; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular and Stroke Nursing, and Council on Epidemiology and Prevention: Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013; 128: 873–934
15) JCS Joint Working Group: Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ J 2014; 78: 2022–2093


This page was created on 2020-03-23T15:26:49.9+09:00
This page was last modified on 2020-04-24T14:20:54.000+09:00
このサイトは(株)国際文献社によって運用されています。