小児体外式膜型人工肺装置の現状An Overview of Pediatric Extracorporeal Membrane Oxygenation
兵庫県立こども病院心臓血管外科Department of Cardiovascular Surgery, Kobe Children’s Hospital ◇ Kobe, Japan
発行日:2020年6月1日Published: June 1, 2020
小児呼吸循環不全患者に対する体外式膜型人工肺装置(ECMO)の歴史は古く,確立された補助手段である.その対象は心疾患症例の急性循環不全のみならず,種々の呼吸器感染症や敗血症,蘇生補助装置としても適応は拡大している.また重度の心機能低下例や高度低酸素血症例に対してもカニュレーションの工夫により一定の効果を得ている.しかしながら,右心バイパス症例のように依然救命困難な疾患群は存在し,比較的合併症のリスクが高い治療法であるため,救命例においてもしばしば神経学的合併症などが問題となる.ECMOによる更なる救命率の向上と合併症回避のためには,近年の成績の概要,新たな知見を集積するとともに,多職種を交えた導入シミュレーション等の体制整備が必須である.
Extracorporeal membrane oxygenation (ECMO) has been the mainstay of short-term pediatric mechanical circulatory support. ECMO can be used to support any form of cardiorespiratory dysfunction. Moreover, an optimal cannulation strategy according to the patient size and underlying condition maximize its safety and efficacy. However, ECMO support in specific patient populations, such as those who have undergone bidirectional Glenn procedure or Fontan procedure, remains challenging. Thus, clear understanding of the short- and long-term results and establishment of active interprofessional ECMO programs are essential for further improvement of ECMO support.
Key words: extracorporeal membrane oxygenation; Extracorporeal Life Support Organization; extracorporeal cardiopulmonary resuscitation
© 2020 特定非営利活動法人日本小児循環器学会© 2020 Japanese Society of Pediatric Cardiology and Cardiac Surgery
小児に対する補助循環装置は体外式膜型人工肺装置(extracorporeal membrane oxygenation: ECMO)と補助人工心臓(ventricular assist device: VAD)に大別される.小児に対するECMO補助の歴史は古く,1973年には初の救命例が報告され1),以後循環補助,呼吸補助に加え蘇生補助手段としても普及している.小児VADに関しては,Berlin Heart EXCOR(Berlin Heart AG, Berlin, Germany)が2015年6月には本邦でも保険償還され,極めて良好な成績を保ち経過しているが,多くの施設では依然補助循環の中心的役割はECMOが担っており,本稿ではECMOの現状として国際レジストリーであるExtracorporeal Life Support Organization(ELSO)からの報告の概要,疾患および管理上の問題点について概要を述べる.
ECMOポンプに必要とされる特徴は,体格に応じた流量の調節性,生体適合性,耐久性,機動性が挙げられる.ポンプには主にローラーポンプと,遠心ポンプがあり,ELSOの統計においても2005年時にはローラーポンプが7割以上を占めていたが,2015年には1割程度にまで減少している2).ローラーポンプの利点としては新生児などに対する低流量での調節性に優れ,遠心ポンプに比べ溶血が少ないが,欠点としては長期的使用において回路破裂の危険性がある.またローラーポンプでは脱血回路の過度の陰圧化を回避するために,ポンプ前回路内に脱血チャンバーと過度の陰圧に対する血流制御装置が必要である.一方遠心ポンプはかつて回転軸周囲での発熱や,血栓形成による溶血や耐久性が問題となっていたが,近年ピボットベアリングシステムにより長期補助が可能となりつつある.モノピボット式ではRotaflow(Maquiet Cardiopulmonary AG, Hirrlingen, Germany),メラ遠心ポンプ(Senko Medical Instrument Mfg. Co., Ltd., Tokyo, Japan),ダブルピボット式のGyroPump(Medtronic, Minneapolis, MN),Capiox SL45(Terumo Corporation, Tokyo, Japan)が臨床使用されている.欧米で体外設置型遠心ポンプのCentriMag(Abbott Laboratories, Abbott Park, IL)などで用いられている磁気浮上型はより血栓,溶血のリスクが低く,高耐久性のポンプである.
小児ECMOの人工肺に求められる特徴は,小型化,抗血栓性生体適合性の向上,低い肺内抵抗,プライミング時の気泡除去の容易さ,酸素添加性能の向上,炭酸ガス除去性能の向上が挙げられる3).かつて人工肺には主にシリコンラバーが用いられており,ELSOの統計においても2005年時には全体の6割以上を占めていたが,その後割合は急激に減少し,代わってpolymethylpentene(PMP)製の中空糸ファイバーがその大半を占めるようになっている2).PMPの特徴として,ガス交換能に極めて優れることから低容量化,炎症反応の低減が可能で,プラズマリークが少なく,血流路の圧力損失が少なく遠心ポンプにも適している.PMPを用いた人工肺として,Qadrox iD(Maquiet Cardiopulmonary AG, Hirrlingen, Germany)やHilite LT(Medos, Stolberg, Germany),CAPIOX LX(Terumo Corporation, Tokyo, Japan)などがある.一方国産のNipro Biocube(Nipro, Osaka, Japan)はpolyolefinにヘパリンコーティングを施し長期使用を可能としている.
圧力センサは3か所での測定が望ましい(Fig. 1).ポンプ前脱血圧は循環血液量を反映し,過度の陰圧を回避する上で必要であり,人工肺後送血圧はカニューレの先当たり等送血路の閉塞を検出する.また人工肺前後の圧力センサにより人工肺抵抗値の推移が把握可能となる.
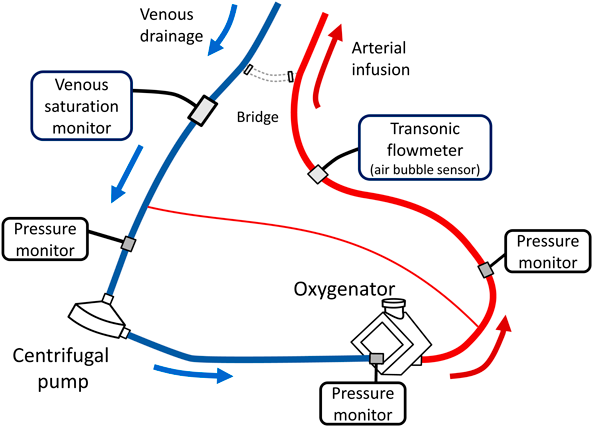
小児ECMOではシャント回路を要することもあり,患者側送血路での流量計設置が必要である.超音波流量計は気泡検出機能も備える.
人工肺でのガス交換効率,酸素供給量,補助血流量を評価する上で有用である.
小児ECMO補助は心臓外科周術期循環補助のみならず,様々な呼吸循環不全が適応となっており,症例の概要については,1989年に発足されたELSOの統計を参考にする4).2016年の報告では7年間に227施設から18歳未満の小児21,907例が登録され,補助目的としておよそ半数が呼吸補助で残りが循環補助あるいは体外循環式心肺蘇生(extracorporeal cardiopulmonary resuscitation: ECPR)の症例であった.疾患カテゴリーによる生存率は7年間概ね横ばいで推移し,新生児呼吸補助,小児呼吸および循環補助症例の生存退院率が60%前後と比較的良好であるのに対し,新生児循環補助およびECPR,小児ECPR症例の生存退院率は45%前後と不良であった4)(Table 1).
| Number of Cases | Survived ECMO (%) | Survived to Hospital Discharge (%) | |
|---|---|---|---|
| Neonatal | |||
| Respiratory | 6,586 | 5,330 (81) | 4,444 (67) |
| Cardiac | 3,285 | 2,258 (69) | 1,487 (45) |
| ECPR | 1,045 | 716 (69) | 445 (43) |
| Pediatric | |||
| Respiratory | 3,903 | 2,732 (70) | 2,353 (60) |
| Cardiac | 4,581 | 3,389 (74) | 2,600 (57) |
| ECPR | 2,507 | 1,471 (59) | 1,066 (43) |
| Total | 21,907 | 15,896 (73) | 12,394 (59) |
| ECMO=extracorporeal membrane Oxygenation. Reprinted from Reference 2) | |||
疾患別で見ると,循環補助においては乳児期以降の心筋炎の生存退院率は75%と他の循環器疾患群に比して良好であった.小児呼吸補助では急性呼吸窮迫症候群(acute respiratory distress syndrome: ARDS)や重症インフルエンザ感染に代表される種々の感染症が適応となり概ね60%台の生存退院率であるのに対し,重症百日咳では生存退院率32%と際立って不良であり,その後のDomicoらによる百日咳に対するECMO補助200例の検討においても,肺高血圧合併例での救命は極めて困難であり5),ECMO単独での治療の限界と,ECMO導入前の白血球除去療法の重要性が示唆されている5, 6).
また,小児呼吸補助症例の増加に伴いその手段としてvenovenous(VV)-ECMOの頻度が2009年の41%から2015年の59%へと経年的に増加を認めている4).本邦ではヨストラ体外循環肺補助用カニューレN®ダブルルーメン(Jostra VVDL; Maquet Getinge group, Germany)が2015年初頭から輸入停止となって以降暫く承認されたダブルルーメンカテーテルがない状況が続いたが,2018年2月にAvalon® Cannula(Avalon Laboratories, Grand Rapids, MI, USA)が承認を得ている.Avalon® Cannulaはワイヤー補強によりカテーテルの虚脱を防ぎ,recirculationが少ない特性を有するが,近年右心系穿孔の頻度が4~15%と報告されており,X線透視,経食道心エコー等を用い確実に適正位置に挿入することが肝要である7).
近年成人のみならず8),小児においても従来の心肺蘇生(cardiopulmonary resuscitation: CPR)に対するECMOを用いたECPRの有用性は実証されており,2016年Lasaらによる多施設レジストリー登録データの解析では,小児院内心肺停止例13,814例を用いpropensity score matchingを行った結果,ECPR群は従来のCPR群に対し生存退院(オッズ比:1.70),神経学的予後(オッズ比:1.78)共に良好であった9).小児ECPRに関する代表的な文献をTable 2に示す10–13).
| Reference (Source) | No. of Patients | % Survival | Factors Associated with Worse Outcome |
|---|---|---|---|
| Chan et al8) (ELSO) | 492 | 42% | single ventricle, history of a stag 1 procedure, acidosis (pH <7.01) |
| Kane et al9) (Boston) | 172 (cardiac) | 51% | non cardiac anomalies, blood prime, acidosis (<7.00), CNS injurey, renal failure, liver injury, ECMO duration≥174 hr, peak post-ECMO lactate (>13 mmol/L) |
| Raymond et al10) (AHA national registry) | 199 | 44% | renal insufficiency, metabolic/electrolyte abnormality, Sodium bicarbonate or tromethamine use |
| McMullan DM et al11) (ELSO) | 641 (neonate) | 39% | low birth wight, PaO2, CNS hemorrhage, pulmonary hemorrhage, acidosis, renal replacement therapy, mechanical compliactions |
| AHA=American Heart Association, ECMO=extracorporeal membrane oxygenation, ELSO=Extracorporeal Life Support Organization, CNS=central nervous system | |||
一方,小児においてはECMO導入に至る蘇生時間と予後の関係についてのコンセンサスは得られていない.Sivarajanらによる単施設報告において30分以上のCPR症例ではそれ以下の症例に対し生存退院率は不良(オッズ比:0.21)であったが14),Raymondらによる多施設レジストリーデータの解析ではECMO導入前の蘇生時間は死亡の危険因子とはならなかった12).小児では患者背景が多様であるが,鼠径アプローチが可能で安定した心臓マッサージが期待できる成人とは異なり,ECMO導入前の蘇生の質も予後に影響し得る.Taebらによる観察研究ではECPR導入例では従来のCPR症例に比べ心臓マッサージが過度に早く,呼気二酸化炭素濃度も低い結果となり,心臓マッサージの質の低下を指摘している15).ECPRの質改善には多職種参加でのシミュレーションが必須で,Sawyerらは認知タクス分析(Cognitive Task Analysis)を用いECPRシミュレーション参加者の認知的問題点の抽出から解決策へと導き,その結果ECPRプロトコル遵守率の改善を報告している16).
高度の心原性ショック例においてはECMO導入後に脈圧の消失,大動脈弁の閉鎖,左室の緊満,高度の肺欝血を来すことがある.ECMO導入後は送血圧により後負荷は増大するため,収縮力の低下した左室では後負荷に打ち勝って駆出することができない.更に補助循環中であっても大動脈弁逆流,脱血しきれない静脈還流,気管支動脈を介した血流,Thebesian veinからの還流血などが左室には流入するため,大動脈弁の開放が得られなくなると速やかに左室の緊満が進む17).左室緊満は心筋障害を助長し,心機能回復を阻害する.加えて肺欝血,肺出血はECMO管理を困難にし,離脱を阻害する.小児では比較的早く1990年前半より左室緊満は問題視され,経皮的心房中隔裂開術や18),引き続いての左房カテーテル留置,小切開を含む外科的な左房脱血など様々な左心系減圧手技が報告されている19–21).我々は劇症型心筋炎症例には頚部アプローチにてECMOを導入した上で,左心系減圧時には左小開胸にて左心耳より脱血管を追加している21)(Fig. 2).また,成人領域においては近年IMPELLA補助循環用ポンプカテーテルを用いたECMO中の左室減圧(いわゆるECPELLA)の有用性も報告されている.左室拡張期圧を下げ,左室内での滞留を回避する点では有用であるが22),小型のIMPELLA 2.5®で,12 Frのポンプ外径,35 mmの大動脈弁下挿入長,52 mm以上の大動脈弓径等の制約があり,現時点での小児におけるECPELLAの報告は限られている23).
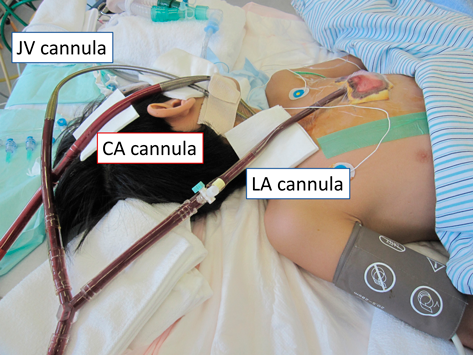
An additional venous cannula was inserted into the left atrial appendage through a left anterior minithoracotomy. The additional cannula was connected to the venous line with Y connector.
Norwood手術後に対するECMO補助はおよそ10~20%の症例に必要と報告されている24, 25).SherwinらによるELSO登録738例の報告では生存退院率は31%であり,2000年から2009年にかけての10年間で明らかな生存率の改善は認められていない26).ECMOの適応により予後は異なるとされ,Allanらの報告ではシャント閉塞等の低酸素血症に対するECMOの生存退院率は81%に対し,循環不全に対しては29%と不良であった24).ECMO中の管理について,体肺動脈短絡術の症例に対してはシャントの取り扱いが問題となる.2000年にJaggersらがECMO補助中にシャントを閉塞させた4例が全例死亡したと報告して以来27),補助中のシャント閉塞を推奨する報告はなく,シャントを介した肺血流を加味し,150~200 mL·kg-1·min-1と高流量での補助を行い,その状態で体血流が維持できない症例のみクリップ等によるシャントの血流制御が推奨されている28).一方,右室肺動脈シャント症例に対するシャントの取り扱い,補助循環血流量に関し,統一の見解は得られていない.
近年本邦では両側肺動脈絞扼術が初回手術として普及しているが,hybrid stage 1 palliation後のECMO補助についての報告は少なく,RoeleveldらのELSO登録44例の報告では生存退院率16%と極めて不良であった29).一因としてhybrid stage 1 palliationの状態では上行大動脈径,大動脈縮窄の程度が症例によって異なり,体循環および冠循環への循環補助の不確実性が推察される.とりわけ頚部アプローチ17例中生存退院は僅かに1例であり,現時点では正中アプローチが妥当と思われる29).
また,循環補助中の両側肺動脈絞扼での血流調整に関しても現時点では明確な指針はない.
機能的単心室に対するECMO補助の報告の大半はStage 1前後の症例で,Glenn手術,Fontan手術後の報告は限られている.2002年にNielsenらによりGlenn手術後の重症RSウイルス感染に対するECMOによる救命例の報告は認めるものの30),2004年のBoothらの報告でGlenn手術後6例中救命例は神経学的後遺症を残した1例のみで31),Alsoufiらの報告でもGlenn手術後ECMO症例の救命率は0%であり32),本疾患群に対するECMOによる救命は極めて困難と考えられていた.
しかしながら2014年のJolleyらによるELSO登録103例の報告では,生存退院率41%と同年代のECMOによる循環補助全体の49%に比べてやや劣るものの従来の報告よりはるかに良好であり,神経学的合併症の頻度も23%と他の疾患群に対し遜色ない成績であった33).ただし,ECMO導入時期についての記載はなく,開胸アプローチが89例と大半はGlenn手術後早期の導入と推察される.また右頸動脈送血5例全例が死亡していることから,術後急性期を過ぎた症例の救命は依然困難と言える.
Glenn循環の特異性として上下大静脈が分離されており,1本の脱血では十分な脱血量が得られない上に,頸静脈脱血では脱血管の挿入長に制限がある.また右心バイパス術後症例の共通点として心臓マッサージによる脳灌流維持は限定的とされる34).Boothらは2本脱血の際には早期脳静脈鬱滞のために上大静脈脱血の先行を推奨しているものの31),これを実証する報告はない.しかし2019年にYoneyamaらはGlenn術後遠隔期の心室頻拍を伴った心筋炎に対し,頸部アプローチでECMOを導入した後,速やかに心窩部アプローチでの右房脱血を追加することでの救命例を報告しており35),術後遠隔期症例には考慮すべき手順と思われる.
Fontan術後もECMO補助は困難とされる.2004年Boothらによる単施設報告では50%の生存退院率が報告されているが31),2011年のRoodらによるELSOデータベース239例の報告では生存退院率35%と他の疾患群に比べ救命率は低い36).ECMO導入においては基本的二心室症例と同様のアプローチが可能であるものの,1本脱血では十分な脱血量が得られず,臓器保護のためにも脱血管の追加が必要となる場合がある.しかしながら静脈閉塞等解剖学的な制約もあり,症例毎の対応を要する31).Fontan術後も上述の如く心肺蘇生の有効性は乏しく,Roodらの報告では心肺蘇生例の生存退院率は25%と更に低下する36).またFontan術後循環不全は時期によって病態,ECMOの有用性は大きく異なる.術後急性期に改変し得る病変を有する症例,一過性の循環不全例で早期離脱の見込める症例はECMOの良い適応とされるが,遠隔期のECMOの位置付けは急変時の短期間補助に留まる34).
ECMOは短期呼吸循環補助を目的とし設計されているが,諸般の事情により長期補助を余儀なくされる場合がある.循環補助目的の長期ECMOについては,92日間の補助循環からの離脱報告は認めるものの37),一般的に成績は不良である.Guptaらによる長期ECMO補助(≧28日)を要した小児22例中10例(45%)は離脱に至ったが,長期生存は3例のみで,かつ2例には重篤な神経学的後遺症を認めている38).また,MerrillらによるELSOデータベースを用いた長期循環補助(≧14日,777例)の解析では,全体の生存退院率は23%で,28日以上の症例の生存退院率は13%と極めて不良であった39).
呼吸補助においては,移植待機,重症呼吸器感染や急性呼吸促拍症候群からの回復に長期補助を要することがある.Broganらによる389例(≧21日)のELSOデータベース症例の解析では生存退院率は38%と循環補助に比べれば良好で40),多臓器不全を合併しない場合の長期補助は妥当とされ,小児では158日間のVV-ECMOからの離脱例も報告されている41).
一方でECMO補助が長期化すると,致死的合併症はないものの,次第に多臓器不全が進行し,回復の見込みがない状況に遭遇することがある42).このような状況下では家族,および医療者に苦渋の決断を迫られ,お互いが受ける精神的ストレスは計り知れない.ECMO補助下に終末期を迎える患児に対する明確な倫理指針は僅かで42),各学会から報告されている終末期医療に関する提言43)や各施設での倫理指針に沿いながら,多職種が加わった医療チームで医学的判断を行い,透明性を保った上で家族と共に患児の終末期医療を進める必要がある.
小児ECMO補助に伴う頭蓋内出血,脳梗塞,癲癇といった急性期神経学的合併症の発生頻度は10~20%と報告されている44).神経学的合併症のリスクファクターとして早産児,低体重,頸動脈カニュレーション,先天性心疾患,心不全,導入前心停止,凝固異常,補助中の状態不安定,回路トラブル等が報告されている44).手技的なものとして頸動脈カニュレーションによる血流障害が危惧されているものの一定の見解は得られていない.Teeleらによる小児ELSO登録2,977例を用いた検討では多変量解析にて頸動脈カニュレーションは他のアプローチに対し神経障害のリスクファクター(オッズ比1.3)であったが45),後のJohnsonらによる小児ELSO登録30,282例を用いた解析では,年齢,性別,体重,人種,Oxygenation Index,導入前心停止,補助様式を調整した結果,頸動脈カニュレーションによる神経学的合併症発生頻度は正中アプローチ,鼠径アプローチに加えVV ECMOとも同等であった46).理論上はWillis動脈輪の形成不全の頻度は6%と報告されており47),そのような症例に対する頸動脈カニュレーションは問題となり得るが,頸動脈カニュレーション側と,脳合併症の左右局在性についても右側が多いとする報告と48),むしろ虚血病変は左側に多いとする報告49)が混在し,結論に至っていない.
小児ECMO症例における遠隔期神経発達に関する代表的な報告をTable 3に示す50–53),発達過程において,IQは正常範囲に保たれていても注意力欠如や言語記憶,視空間記憶といった特定の機能が問題となる点,MRIでは海馬の容積低下と言語記憶の関与,白質の異方性比率(fractional anisotropy)の低下と注意障害との関連などが指摘されている54).また,ECMO後の神経発達に関する問題は成長と共に顕在化するとされ,長期的なフォローアップが必要である55).評価においてToussaintらは新生児ECMO生存者を8歳時に評価した結果,22%の症例に運動機能的問題があるにもかかわらず自己評価がむしろ健常者より高くなる傾向を指摘しており,問診のみならず,客観的機能評価の重要性を指摘している56).
| Reference | Patient Population | Neurological evaluation | ||
|---|---|---|---|---|
| Age | Methods of evaluation | Results | ||
| McNally et al42) | neonatal respiratory: 56 | 7 yeas | British Ability Scales II (BAS), Movement Assessment Battery for Children (MABC) | mild disability: 23% |
| moderate disability: 16% | ||||
| severe disability: 5% | ||||
| Wanger et al43) | cardiac: 13, respiratory: 9 | 7.2 years | Bayley Scales of Infant Development (BSID II), Wechsler Preschool and Primary Scale of Intelligence Revised (WPSSI-R), Neuropsychologic Assessment (NEPSY), Wechsler Intelligence Scale for Children III (WISC III) | mild-moderate impairment: 45.4% |
| severe impairment: 27.3% | ||||
| Lequier et al44) | cardiac: 16 | 53 months | Bayley Scales of Infant Development, mental scale, Wechsler Preschool and Primary Scale of Intelligence | mental delay: 50% |
| motor or sensory diability: 12.5% | ||||
| Chrysostomou et al45) | cardiac: 63 | Pediatric Overall Performance Category (POPC), Pediatric Cerebral Performance Category (PCPC) | mild disability: 22.2% | |
| moderate disability: 9.5% | ||||
| severe disability: 1.6% | ||||
小児補助循環としてのECMOの概要を述べた.ECMOは本邦でも多くの小児施設で使用可能である一方,欧米に比して一施設当たりの導入数は少なく,循環以外でECMOにより救命できる症例が潜在している可能性がある.今後本邦においても小児集中治療部門の更なる普及に伴い,様々な疾患がECMOの適応となることが予想され,適応に関する知識のアップデートは必要である.現時点での小児ECMOの問題点を認識した上での治療戦略により,今後更なる救命率向上と合併症回避を願い本稿を終える.
本稿において開示すべき利益相反はありません.
1) Soeter JR, Mamiya RT, Sprague AY, et al: Prolonged extracorporeal oxygenation for cardiorespiratory failure after tetralogy correction. J Thorac Cardiovasc Surg 1973; 66: 214–218
2) Toomasian JM, Vercaemst L, Bottrell S, et al: The circuit, in Brogan TV (ed): Extracorporeal Life Support: The ELSO Red Book. Extracorporeal Life Support Organization, Ann Arbor, Michigan, 2017, pp 49–80
3) 片桐伸将:人工肺.人工臓器2010; 39: 170–173
4) Barbaro RP, Paden ML, Guner YS, et al: ELSO member centers: Pediatric extracorporeal life support organization registry international report 2016. ASAIO J 2017; 63: 456–463
5) Domico M, Ridout D, MacLaren G, et al: Extracorporeal membrane oxygenation for pertussis: Predictors of outcome including pulmonary hypertension and leukodepletion. Pediatr Crit Care Med 2018; 19: 254–261
6) Rowlands HE, Goldman AP, Harrington K, et al: Impact of rapid leukodepletion on the outcome of severe clinical pertussis in young infants. Pediatrics 2010; 126: e816–e827
7) Berdajs D: Bicaval dual-lumen cannula for venovenous extracorporeal membrane oxygenation: Avalon© cannula in childhood disease. Perfusion 2015; 30: 182–186
8) Chen YS, Lin JW, Yu HY, et al: Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: An observational study and propensity analysis. Lancet 2008; 372: 554–561
9) Lasa JJ, Rogers RS, Localio R, et al: Extracorporeal cardiopulmonary resuscitation (E-CPR) during pediatric in-hospital cardiopulmonary arrest is associated with improved survival to discharge: A report from the American Heart Association’s Get With The Guidelines-Resuscitation (GWTG-R) Registry. Circulation 2016; 133: 165–176
10) Chan T, Thiagarajan RR, Frank D, et al: Survival after extracorporeal cardiopulmonary resuscitation in infants and children with heart disease. J Thorac Cardiovasc Surg 2008; 136: 984–992
11) Kane DA, Thiagarajan RR, Wypij D, et al: Rapid-response extracorporeal membrane oxygenation to support cardiopulmonary resuscitation in children with cardiac disease. Circulation 2010; 122 Suppl: S241–S248
12) Raymond TT, Cunnyngham CB, Thompson MT, et al: American Heart Association National Registry of CPR Investigators: Outcomes among neonates, infants, and children after extracorporeal cardiopulmonary resuscitation for refractory inhospital pediatric cardiac arrest: A report from the National Registry of Cardiopulmonary Resuscitation. Pediatr Crit Care Med 2010; 10: 362–371
13) McMullan DM, Thiagarajan RR, Smith KM, et al: Extracorporeal cardiopulmonary resuscitation outcomes in term and premature neonates*. Pediatr Crit Care Med 2014; 15: e9–e16
14) Sivarajan VB, Best D, Brizard CP, et al: Duration of resuscitation prior to rescue extracorporeal membrane oxygenation impacts outcome in children with heart disease. Intensive Care Med 2011; 37: 853–860
15) Taeb M, Levin AB, Spaeder MC, et al: Comparison of pediatric cardiopulmonary resuscitation quality in classic cardiopulmonary resuscitation and extracorporeal cardiopulmonary resuscitation events using video review. Pediatr Crit Care Med 2018; 19: 831–838
16) Sawyer T, Burke C, McMullan DM, et al: Impacts of a pediatric extracorporeal cardiopulmonary resuscitation (ECPR) simulation training program. Acad Pediatr 2019; 19: 566–571
17) Cevasco M, Takayama H, Ando M, et al: Left ventricular distension and venting strategies for patients on venoarterial extracorporeal membrane oxygenation. J Thorac Dis 2019; 11: 1676–1683
18) Koenig PR, Ralston MA, Kimball TR, et al: Balloon atrial septostomy for left ventricular decompression in patients receiving extracorporeal membrane oxygenation for myocardial failure. J Pediatr 1993; 122: S95–S99
19) Hlavacek AM, Atz AM, Bradley SM, et al: Left atrial decompression by percutaneous cannula placement while on extracorporeal membrane oxygenation. J Thorac Cardiovasc Surg 2005; 130: 595–596
20) del Nido PJ, Armitage JM, Fricker FJ, et al: Extracorporeal membrane oxygenation support as a bridge to pediatric heart transplantation. Circulation 1994; 90: II66–II69
21) Yamamoto M, Oshima Y, Matsuhisa H, et al: Left atrial decompression by minithoracotomy during extracorporeal life support. Ann Thorac Surg 2019; 107: e227–e228
22) Dickstein ML: The starling relationship and veno-arterial ECMO: Ventricular distension explained. ASAIO J 2018; 64: 497–501
23) Dimas VV, Morray BH, Kim DW, et al: A multicenter study of the impella device for mechanical support of the systemic circulation in pediatric and adolescent patients. Catheter Cardiovasc Interv 2017; 90: 124–129
24) Allan CK, Thiagarajan RR, del Nido PJ, et al: Indication for initiation of mechanical circulatory support impacts survival of infants with shunted single-ventricle circulation supported with extracorporeal membrane oxygenation. J Thorac Cardiovasc Surg 2007; 133: 660–667
25) Debrunner MG, Porayette P, Breinholt JP 3rd, et al: Midterm survival of infants requiring postoperative extracorporeal membrane oxygenation after Norwood palliation. Pediatr Cardiol 2013; 34: 570–575
26) Sherwin ED, Gauvreau K, Scheurer MA, et al: Extracorporeal membrane oxygenation after stage 1 palliation for hypoplastic left heart syndrome. J Thorac Cardiovasc Surg 2012; 144: 1337–1343
27) Jaggers JJ, Forbess JM, Shah AS, et al: Extracorporeal membrane oxygenation for infant postcardiotomy support: Significance of shunt management. Ann Thorac Surg 2000; 69: 1476–1483
28) Dalton HJ, Tucker D: Resuscitation and extracorporeal life support during cardiopulmonary resuscitation following the Norwood (Stage 1) operation. Cardiol Young 2011; 21 Suppl 2: 101–108
29) Roeleveld PP, Wilde R, Hazekamp M, et al: Extracorporeal membrane oxygenation in single ventricle lesions palliated via the hybrid approach. World J Pediatr Congenit Heart Surg 2014; 5: 393–397
30) Nielsen JC, Seiden HS, Nguyen K, et al: Extracorporeal membrane oxygenation for pneumonitis after a Glenn palliation. Perfusion 2002; 17: 457–458
31) Booth KL, Roth SJ, Thiagarajan RR, et al: Extracorporeal membrane oxygenation support of the Fontan and bidirectional Glenn circulations. Ann Thorac Surg 2004; 77: 1341–1348
32) Alsoufi B, Awan A, Manlhiot C, et al: Does single ventricle physiology affect survival of children requiring extracorporeal membrane oxygenation support following cardiac surgery? World J Pediatr Congenit Heart Surg 2014; 5: 7–15
33) Jolley M, Thiagarajan RR, Barrett CS, et al: Extracorporeal membrane oxygenation in patients undergoing superior cavopulmonary anastomosis. J Thorac Cardiovasc Surg 2014; 148: 1512–1518
34) Bacon MK, Gray SB, Schwartz SM, et al: Extracorporeal membrane oxygenation (ECMO) support in special patient populations: The bidirectional Glenn and Fontan circulations. Front Pediatr 2018; 6: 299
35) Yoneyama F, Okamura T: Quick atrial access by subxiphoid approach in extracorporeal cardiopulmonary resuscitation after bidirectional Glenn procedure. Perfusion 2019; 34: 425–427
36) Rood KL, Teele SA, Barrett CS, et al: Extracorporeal membrane oxygenation support after the Fontan operation. J Thorac Cardiovasc Surg 2011; 142: 504–510
37) Bilal MS, Avsar MK, Yıldırım Ö, et al: Ninety-two days of extracorporeal membrane oxygenation support following congenital heart surgery. Perfusion 2017; 32: 514–516
38) Gupta P, McDonald R, Chipman CW, et al: 20-year experience of prolonged extracorporeal membrane oxygenation in critically ill children with cardiac or pulmonary failure. Ann Thorac Surg 2012; 93: 1584–1590
39) Merrill ED, Schoeneberg L, Sandesara P, et al: Outcomes after prolonged extracorporeal membrane oxygenation support in children with cardiac disease: Extracorporeal Life Support Organization registry study. J Thorac Cardiovasc Surg 2014; 148: 582–588
40) Brogan TV, Zabrocki L, Thiagarajan RR, et al: Prolonged extracorporeal membrane oxygenation for children with respiratory failure. Pediatr Crit Care Med 2012; 13: e249–e254
41) Maeda K, Ryan K, Conrad CK, et al: An alternative cannulation approach for venovenous extracorporeal membrane oxygenation in children for long-term ambulatory support. J Thorac Cardiovasc Surg 2018; 156: e13–e14
42) Kirsch R, Munson D: Ethical and end of life considerations for neonates requiring ECMO support. Semin Perinatol 2018; 42: 129–137
43) 日本循環器学会:循環器疾患における末期医療に関する提言.2011; www.j-circ.or.jp/guideline/pdf/JCS2010_nonogi_h.pdf
44) Lorusso R, Taccone FS, Belliato M, et al: Euro-ELSO Working Group on Neurologic Monitoring and Outcome: Brain monitoring in adult and pediatric ECMO patients: The importance of early and late assessments. Minerva Anestesiol 2017; 83: 1061–1074
45) Teele SA, Salvin JW, Barrett CS, et al: The association of carotid artery cannulation and neurologic injury in pediatric patients supported with venoarterial extracorporeal membrane oxygenation. Pediatr Crit Care Med 2014; 15: 355–361
46) Johnson K, Jarboe MD, Mychaliska GB, et al: ELSO/Euro-ELSO Neurologic Outcomes Working Group: Is there a best approach for extracorporeal life support cannulation: A review of the extracorporeal life support organization. J Pediatr Surg 2018; 53: 1301–1304
47) Iqbal S: A comprehensive study of the anatomical variations of the circle of willis in adult human brains. J Clin Diagn Res 2013; 7: 2423–2427
48) Pinto VL, Pruthi S, Westrick AC, et al: Brain magnetic resonance imaging findings in pediatric patients post extracorporeal membrane oxygenation. ASAIO J 2017; 63: 810–814
49) Raets MM, Dudink J, Ijsselstijn H, et al: Brain injury associated with neonatal extracorporeal membrane oxygenation in the Netherlands: A nationwide evaluation spanning two decades. Pediatr Crit Care Med 2013; 14: 884–892
50) McNally H, Bennett CC, Elbourne D, et al: UK Collaborative ECMO Trial Group: United Kingdom collaborative randomized trial of neonatal extracorporeal membrane oxygenation: Follow-up to age 7 years. Pediatrics 2006; 117: e845–e854
51) Wagner K, Risnes I, Berntsen T, et al: Clinical and psychosocial follow-up study of children treated with extracorporeal membrane oxygenation. Ann Thorac Surg 2007; 84: 1349–1355
52) Lequier L, Joffe AR, Robertson CM, et al: Western Canadian Complex Pediatric Therapies Program Follow-up Group: Two-year survival, mental, and motor outcomes after cardiac extracorporeal life support at less than five years of age. J Thorac Cardiovasc Surg 2008; 136: 976–983.e3
53) Chrysostomou C, Maul T, Callahan PM, et al: Neurodevelopmental outcomes after pediatric cardiac ECMO support. Front Pediatr 2013; 1: 1–6
54) Schiller RM, IJsselstijn H, Madderom MJ, et al: Neurobiologic correlates of attention and memory deficits following critical illness in early life. Crit Care Med 2017; 45: 1742–1750
55) IJsselstijn H, Hunfeld M, Schiller RM, et al: Improving long-term outcomes after extracorporeal membrane oxygenation: From observational follow-up programs toward risk stratification. Front Pediatr 2018; 26: 177
56) Toussaint LC, van der Cammen-van Zijp MH, Janssen AJ, et al: Perceived motor competence differs from actual performance in 8-year-old neonatal ECMO survivors. Pediatrics 2016; 137: e20152724


This page was created on 2020-06-01T15:56:51.148+09:00
This page was last modified on 2020-06-18T09:54:30.000+09:00
このサイトは(株)国際文献社によって運用されています。