胎児心不全:不整脈の重症度をどう評価するAssessment of the Severity of Heart Failure in Fetuses with Fetal Arrhythmias
雪の聖母会聖マリア病院新生児科Department of Neonatology, St. Mary’s Hospital ◇ Fukuoka, Japan
発行日:2019年11月1日Published: November 1, 2019
胎児不整脈では,心不全が進行すると胎児水腫となり胎内死亡をきたすため,心不全の重症度評価は重要な課題となるが,実際には正確な評価は難しい.通常,胎児心エコー検査で胎児心不全を評価するCVP (cardiovascular profiling)スコアなどで使用されるドプラ血流波形は,不整脈により変化するため評価に使用できない項目が多い.そこで,心拡大の程度や房室弁閉鎖不全の出現,特に僧帽弁閉鎖不全に着目したり,血流波形のVTI (velocity-time integral)による心拍出量の算出で心不全の兆候を検出する.胎児の一般的な全身状態の評価であるBPS (biophysical profiling score)も参考にできる.心拍数との関連では,頻脈性不整脈では,上室頻拍では心拍220回/分以上,心室頻拍では200回/分以上,胎児徐脈性不整脈では心拍55回/分未満が心不全進行の目安となる.しかし,不整脈症例では,頻脈時の頻拍源性心筋症の併発や,徐脈時には心奇形や抗SS-A抗体による心筋炎/心筋症の合併によって心機能が低下してくることが知られており,心拍数のみでは心不全進行の予測は不十分である.複数の指標を合わせて,継時的な経過観察により症例ごとの計測値の変化を評価しながら,管理方法を判断していくことが重要である.
Fetal arrhythmia is a known cause of fetal heart failure that can lead to fetal death. Although assessment of the severity of heart failure is important for managing affected fetuses, it is often difficult in fetuses with arrhythmias. Usually, Doppler waveform, which is accepted in the cardiovascular profiling (CVP) score, is the most useful finding for assessing cardiac function. However, arrhythmia changes the Doppler waveform regardless of the cardiac function, so many of these waveforms may not reveal heart failure. Hence, other fetal echocardiographic findings, such as cardiomegaly assessed by the cardiothoracic area ratio, presence of atrioventricular valve regurgitation, and assessment of cardiac output calculated from the velocity-time integral, are used to detect early signs of cardiac failure. The Biophysical Profiling Score is another method useful for assessing the well-being of affected fetuses. Regarding the fetal heart rate, fetuses often develop heart failure with a fetal heart rate >220 bpm in fetal supraventricular tachycardia, >200 bpm in fetal ventricular tachycardia, and <55 bpm in fetal bradycardia. However, most fetuses with arrhythmia also have cardiac dysfunction, such as tachycardia-induced cardiomyopathy in fetal tachycardia and myocarditis caused by anti-SS-A antibody in fetal bradycardia. Hence, fetal heart rate may not reflect the severity of heart failure in many fetuses. Assessment by combining multiple assessment strategies and sequential follow-up of these findings are essential for assessing heart failure in fetuses with arrhythmias.
Key words: fetal arrhythmias; fetal heart failure; fetal echocardiography; fetal tachycardia; fetal bradycardia
© 2019 特定非営利活動法人日本小児循環器学会© 2019 Japanese Society of Pediatric Cardiology and Cardiac Surgery
胎児不整脈では,心不全が進行すると胎児水腫となり胎内死亡をきたす.したがって心不全の重症度評価は重要な課題となるが,実際には正確な評価は難しい.胎児心エコーでは,通常はドプラ血流波形を使用することが多いが,不整脈があると,波形が不整脈自体により変化するため評価に使用できないことが多い.そのなかで,どのような所見に注目しながら評価して,それぞれの症例の周産期管理を行っていくのか,解説する.
胎児不整脈は,徐脈性不整脈,頻脈性不整脈,およびその他の脈の不整の3つに大きく分類され1–3),この中で徐脈と頻脈のとき胎児心不全の評価が必要となる.徐脈性不整脈は,胎児心拍数が100回/分未満,頻脈性不整脈は200回/分以上と定義されることが多い.ただし,頻脈性不整脈では,急激な心拍数の変化などで不整脈の存在が示唆されるときには180回/分以上であれば頻脈性不整脈と定義している文献も多い.胎児期の不整脈診断は,主に心エコー検査によって行う.Mモード法(Fig. 1),ドプラ法による心房心室収縮を同時に評価する画像を描出し(Fig. 2),心房心室収縮の関連を見ることで不整脈の診断を行う1–3).
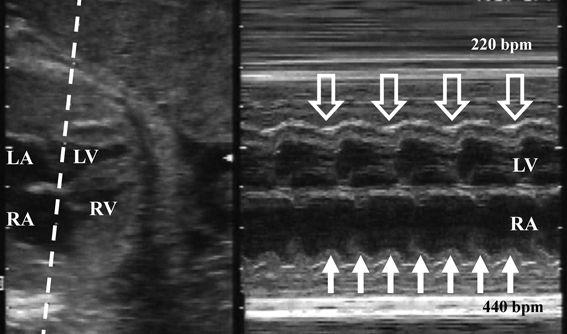
Simultaneous record of the left ventricle (LV) and the right atrium (RA) reveales 2 : 1 relation of atrial (white arrow) and ventricular contraction (hollow arrow). bpm, beats per minute; LA, left ventricle; RV, right ventricle.
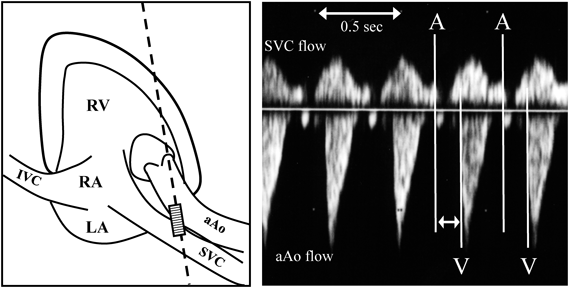
Right panel reveals the wave form of fetuses with normal sinus rhythm. Starting point of small reversal flow at SVC represents the timing of atrial contraction (A), and the starting point of forward flow at aAo represents the timing of ventricular contraction (V). The arrow reveals atrio-ventricular interval. IVC, inferior vena cava; LA, left atrium; RA, right atrium; RV, right ventricle.
徐脈性不整脈では,まれに洞性徐脈もあるが,多くは房室伝導が乖離した完全房室ブロックであり,およそ半数ほどは先天性心奇形(多脾症候群や修正大血管転位など)に起因する.残りの半数ほどは心内構造が正常であり,この場合は母体の抗SS-A抗体に起因していることが多い.抗SS-A抗体陽性母体の1~7%に房室ブロックを発症するが,実際には母体はシェーグレン症候群やSLEは発症しておらず,胎児房室ブロックの発症後検査で抗体陽性に気づかれることが多い.
頻脈性不整脈では,上室頻拍と心房粗動が多く,そのほか心室頻拍もある.上室頻拍は心房心室が1 : 1伝導のものであり,胎児頻脈性不整脈のおよそ2/3を占める.多くが房室回帰性頻拍(WPW症候群)で,その他,異所性心房頻拍や房室結節回帰性頻拍も認める.心房心室が2 : 1で伝導する心房粗動が次に多く,この2つで胎児頻脈の大部分を占める.心室拍数のみ頻拍となる心室頻拍は稀である.頻脈性不整脈では,持続性のものと,間歇的な頻脈があり(Fig. 3),頻脈出現時間が全体の50%以上のときに心不全をきたす危険性が出てくるとされている.
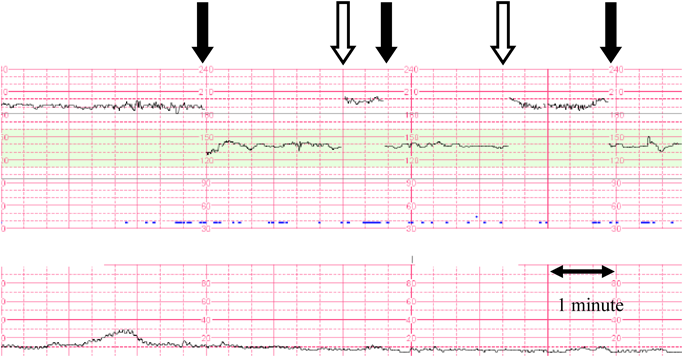
Fetuses with the tachycardic episode more than 50% are thought to be a risk for developing fetal hydrops.
通常,胎児心エコー検査で胎児心不全を評価する時には,CVPスコアが使用されることが多い(Table 1)4).しかし,胎児不整脈のときに問題となるのは,CVPスコアでは6項目中3項目にドプラ血流波形(臍帯静脈,静脈管,臍帯動脈)が使用されている点である.胎児不整脈では,血流波形は心不全の程度にかかわらず不整脈自体により変化してしまう.このため,このCVPスコアそのまま使用することができない.
| Parameter | Cardiovascular Profile Score | ||
|---|---|---|---|
| 0 points | −1 point | −2 points | |
| Hydrops | None | Ascites or pericardial or pleural effusion | Skin edema |
| Ductus venosus and umbilical vein Doppler | DV atrial flow reversal | UV atrial pulsations | |
| Heart size (CTAR: heart area/chest area) | >0.20 to <0.35 | 0.35 to 0.50 | <0.20 or >0.50 |
| Cardiac function | Normal TV and MV, RV and LV SF >0.28, biphasic diastolic filling | Holosystolic TR or MR, RV or LV SF <0.28, ventricular hypertrophy | dP/dT at AV valve <400 or monophasic filling |
| Umbilical artery Doppler | Absent end-diastolic flow with brain sparing | Reversed end-diastolic flow | |
| AV, atrioventricular; CTAR, cardiothoracic area ratio; dP/dT, change in pressure/time; DV, ductus venosus; MR, mitral regurgitation; MV, mitral valve; SF, shortening fraction;TR, tricuspid regurgitation; TV, tricuspid valve; UV, umbilical vein. | |||
静脈の血流波形で心不全を評価する時には,心房収縮時の逆流波が増大するのを指標として使用している.しかし不整脈があると,心不全がなくても,この大きな逆流波が出現する.不整脈では,心房と心室の収縮時相にずれが生じるため,心室が収縮し房室弁が閉鎖しているタイミングで心房が収縮することがある.このとき心房収縮による血流は心室に入ることができず,静脈に向かって大きく逆流する(Fig. 4, 5).
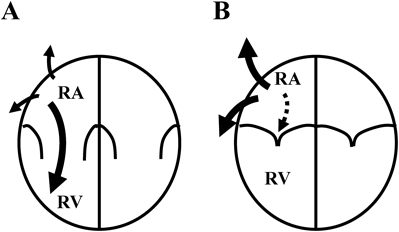
A. In fetuses with normal sinus rhythm, the right atrium (RA) contract during diastolic phase of the right ventricle (RV). Most of the flood flow made by the RA contraction goes into the RV, and only small amount of the flood flow goes back to the vena cava. B. In fetuses with the arrhythmia, RA can contract during systolic phase. In this situation, blood in the RA can not go into the RV since the tricuspid valve is closed. Hence a large amount of the blood go back to the vena cava regardless the cardiac function.
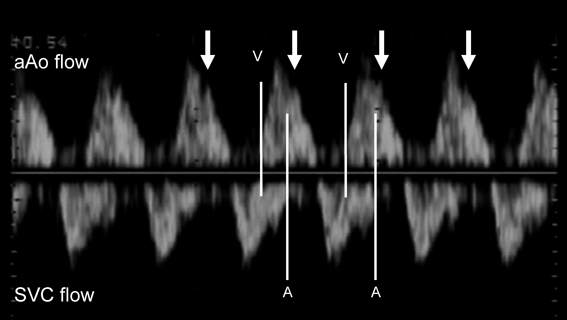
SVC flow reveals large reversal flow (arrow) made by the atrial contraction started at a line A, since the atria contracts during aAo flow which represents the ventricular systolic phase started at a line V.
また,CVPスコアでは,房室弁流入波形が正常の2峰性(E波とA波)から1峰性になることを心不全の指標として使用している.しかし頻脈により心拍数が上昇していると,心不全がなくても1峰性であり,心不全の程度の評価の参考にならない.
したがって,CVPスコアからは,血流波形以外の項目,胎児水腫の程度,心拡大の程度(cardiothoracic area ratio: CTAR)と,房室弁閉鎖不全が,胎児心不全の指標として使用できる項目となる.ただし,臨床的には,心不全による胎児水腫への進行を予見することを求められることが多いため,それ以外のCTARと房室弁閉鎖不全が,評価に有用な所見であろう.
上記の通り,CVPスコアの中にあるCTARと房室弁閉鎖不全があり,そのほか,心エコー検査関連の項目では心拍出量も使用できる.一方,超音波検査以外の所見も合わせた,胎児の全身状態を評価するBiophysical Profile Score(BPS)も心不全の重要な指標となる.
心不全では心拡大をきたすことがよく知られているが,特に胎児不整脈のときにはこの心拡大が心不全の指標として重要な所見となる.これは,胎児頻脈性不整脈では頻脈誘発性心筋症が,胎児徐脈性不整脈では心筋炎/心筋症の発症が急激な心不全の進行に重要な要因となるためである.
頻脈時の心不全の原因では,頻脈自体で1回拍出量が次第に低下し時間当たりの心拍出量が低下することもあるが,より重要なものに頻脈誘発性心筋症がある.頻脈が持続すると拡張型心筋症のごとく心筋が菲薄化し心拡大をきたす.これにより,頻拍の拍数は変わらなくても急激に心不全が進行するため,胎児頻脈症例では心拡大の程度を継時的に評価することが重要となる.
徐脈時は,1回拍出量の増加で心拍出量を維持するために両心室が拡大しているため,もともと少なからず心拡大を認める.しかし,それ以上に重要な要因として,抗SS-A抗体による胎児の心筋炎/心筋症による心拡大がある.胎児房室ブロックのとき高頻度に心筋炎/心筋症が併発しており,心機能が低下し心不全がより悪化する5).したがって,徐脈の症例を管理するときにも,心拡大の程度を継時的に評価する.
心不全では,種々の要因により房室弁閉鎖不全が出現し,さらにこの逆流により心不全も増悪するため,この三尖弁や僧帽弁閉鎖不全は心不全の重要な指標となる3).心不全が増悪してくると,心筋の機能が低下して乳頭筋不全となり,房室弁の閉鎖不全をきたす.また心拡大により弁輪拡大やテザリングのため房室弁閉鎖不全をきたす.したがって房室弁の逆流の出現自体が心不全の指標となる.そしていったん房室弁に逆流が起きると,大血管方向への心拍出量が減少すること,および心房の容量負荷からやがて心房圧が上昇することにより,さらに心不全を悪化させる.このため,房室弁に逆流が認められれば,その後に心不全が増悪してくることが予測される.
房室弁閉鎖不全では,三尖弁閉鎖不全より僧帽弁閉鎖不全のほうが,心不全の指標としては重要となる.正常心機能のときには,僧帽弁閉鎖不全は認められないため,この所見が認められれば左室機能の低下が進行していることが示唆される(Fig. 6).心拡大の項目で示した通り,胎児頻脈性不整脈でも胎児徐脈性不整脈でも心筋の機能低下が心不全増悪の重要な要因となるため,僧帽弁閉鎖不全の出現は重要な指標となる.
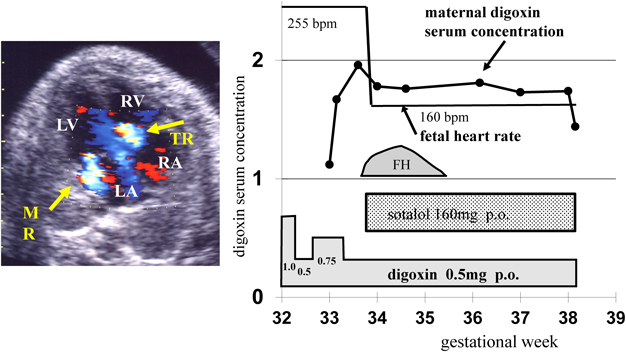
Maternal administration of digoxin was started at 32 weeks of gestation, but the tachycardia persisted. MR was found at 33 weeks of gestation and fetus developed to fetal hydrops (FH) after that. Shortly after adding sotalol, the fetus became to sinus rhythm. Of note, the MR persisted and FH worsened after for a few days of recovery of sinus rhythm, suggested the presence of tachycardia induced cardiomyopathy. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TR, tricuspid regurgitation.
一方,三尖弁閉鎖不全では,胎児期には心機能が正常のときにも高頻度に認められることは知られている.正常時の多くは収縮期早期のみの短い持続のものであるため,全収縮期に認めることを心不全の兆候として使用することもある.しかし正常心でもこの全収縮期の逆流を認めることがあるため,この所見のみで強い心不全があるとは判断できず,経時的な観察で増悪傾向の有無を観察する.
そのほか,房室弁閉鎖不全があるときは,dP/dTが計測できる.胎児期には収縮期圧が低いため,房室弁逆流血流の流速が0.5 m/secから2.5 m/secとなる24 mmHgの変化にかかった時間を計測して算出する.dP/dTが400 mmHg/sec未満が心筋収縮能低下の一つの指標となるが4),これも経時的な変化を評価する.
心エコーでは,ドプラ波形により心拍出量が算出できるため,特に徐脈のときに心拍出量が維持できているかの指標として使用される.ドプラ波形では,(血管の断面積)×(ドプラ波形のVTI)で血流量が算出でき(Fig. 7),これに心拍数を掛けると一分間の心拍出量が算出される.これを大動脈弁部と肺動脈弁部で算出すると両心室からの総心拍出量が得られる.正常では,体重1 kgあたり400 mL/minの総心拍出量がある.心拍出量も1日の計測による絶対値の評価より,継時的な推移を見て判断する.
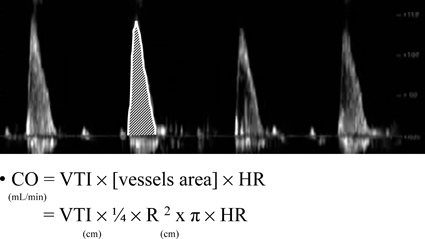
Flow volume of a single beat is calculated from the velocity time integral (VTI) measured by the area of the Doppler signal, multiplied by the area of the vessel (R represents the diameter of the vessel). The flow volume in a minute is calculated by the flow volume in a single beat multiplied by the heart rate (HR). Total cardiac output during fetal period is obtained by adding the flow volume at the aortic valve and the pulmonary valve.
BPSは,産科ではよく使用されている胎児の全身状態を評価するスコアである.スコアとしては超音波検査所見のほか,胎児心拍モニタ所見を使用して算出されるが,胎児不整脈があるときには,胎児心拍モニタの評価が使用できないため,超音波所見からの評価を使用することとなる.とくにすでに胎児水腫へと進行した症例などでは,BPSによる胎児の全身状態の評価を行い,胎児死亡をきたす前に児の娩出による体外治療への移行のタイミングを計るときなど,指標として使用できる.
| Parameter | Normal (2 points) | Abnormal (0 points) |
|---|---|---|
| NST/Reactive FHR | At least two accelerations in 20 minutes | Less than two accelerations to satisfy the test in 20 minutes |
| US: Fetal breathing movements | At least one episode of >30 s in 30 minutes | None or less than 30 s |
| US: Fetal activity/gross body movements | At least three movements of the torso or limbs | Less than three movements |
| US: Fetal muscle tone | At least one episode of active bending and straightening of the limb or trunk | No movements or movements slow and incomplete |
| US: Qualitative amniotic fluid | At least one vertical pocket >2 cm in the vertical axis | Largest vertical pocket </=2 cm |
| FHR, fetal heart rate; NST, non-stress test; US, ultrasound | ||
頻脈性不整脈のときも徐脈性不整脈のときも,上記の通り合併する心機能の低下なども心不全をきたす大きな要因であり,心不全へ進行する心拍数の限界のような値は明確なものはない.しかし,ある程度の参考となる値を知っておくことは,管理をする上で有用であろう.
頻脈性不整脈の時は,上室頻拍では220回/分以上のときに心不全へ進行のリスクが高いとの報告がある1).日常の臨床においても,胎児治療にて上室頻拍を管理しているとき,洞調律に戻らなくても,心拍数がやや低下してレートコントロールされて200回/分近くへ下がってくれば,胎児水腫が徐々に改善する,ということはしばしば経験される.一方,心室頻拍では200回/分以上の,より低い心拍数で心不全へ進行する.
徐脈性不整脈では,55回/分未満という値が心不全へ進行するラインとしてよく使用される.ただし,実際の臨床の場においては,徐脈のときは頻脈のとき以上に,症例により差が大きい.心奇形に伴う徐脈では心不全へ進行する症例が多く,60回/分程度でもリスクが高い.逆に,心奇形を伴わず抗SS-A抗体も陰性の症例では,37回/分まで低下しても胎児水腫へ進行しなかったとの報告もある6).
胎児不整脈では,解説してきたように,どれか一つの指標で正確に心不全を評価できるというものはない.したがって,心拍数や心機能などから心不全へ進行する危険性を判断しながら,複数の指標を使用して心不全の程度を評価する必要がある.そのときには,BPSなどの児の全身状態の指標も併用して評価していく.そしてさらに,継時的な経過観察により,症例ごとの計測値の変化を評価しながら,管理方法を判断していくことが重要である.
本稿に関する利益相反はありません.
1) 里見元義,川滝元良,西畠 信,ほか:胎児心エコー検査ガイドライン.日本循環器学会誌 2006; 22: 591–613
2) Donofrio MT, Moon-Grady AJ, Hornberger LK, et al: American Heart Association Adults With Congenital Heart Disease Joint Committee of the Council on Cardiovascular Disease in the Young and Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Council on Cardiovascular and Stroke Nursing: Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Circulation 2014; 129: 2183–2242
3) 前野泰樹:胎児不整脈.長嶋正實,住友直方,牛ノ濱大也,ほか:小児不整脈.改訂第2版.診断と治療社.東京,2012, pp204–214
4) Huhta JC: Fetal congestive heart failure. Semin Fetal Neonatal Med 2005; 10: 542–552
5) Trucco SM, Jaeggi E, Cuneo B, et al: Use of intravenous gamma globulin and corticosteroids in the treatment of maternal autoantibody-mediated cardiomyopathy. J Am Coll Cardiol 2011; 57: 715–723
6) Vesel S, Završnik T, Podnar T: Succesful outcome in a fetus with an extremely low heart rate due to isolated complete congenital heart block. Ultrasound Obstet Gynecol 2003; 21: 189–191


This page was created on 2019-11-20T11:35:40.103+09:00
This page was last modified on 2019-12-16T14:53:23.000+09:00
このサイトは(株)国際文献社によって運用されています。