1. Balloon Atrial Septostomy(BAS):心房中隔裂開術1)
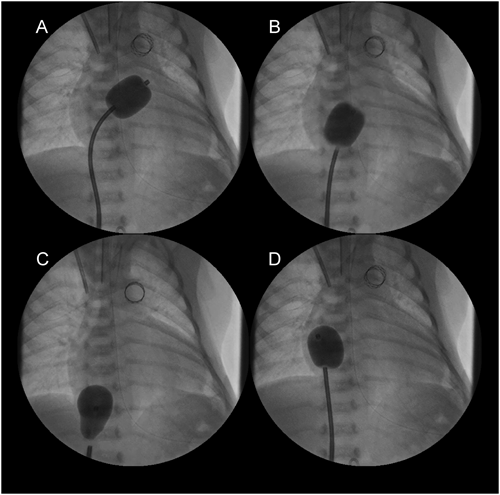
BASの手技(Fig. 1)
房室弁の損傷をきたす可能性があるので必ず正面・側面透視を使用する.右房(RA)内にあるカテーテルを後左方へ向けて左房(LA)へ通す.軽くテストインフレーションして心室に引き込まれないことを確認してから,力まずにスピードを付けてシャフトを手前に短く引く(B).抵抗を感じるが直ぐに下大静脈(IVC)へ入り込むので(C),RAへ押し戻す(D).小さめ(1 ccの注入)から開始し,徐々にサイズアップするのが安全である.
現在日本でBASに保険適応されているカテーテルは2種類ある.Rashkind catheterは最大注入量が2 cc,最大径が14 mm,適合シースは6Fである.一方Miller catheterは最大注入量が4 cc,最大径が19 mmと大きいが,適合シースは7Fである.できる限り大腿静脈(FV)の閉塞を避けるためにRashkind catheterが選択されることが多い.低体重児の場合はさらにFVが細いので,BASには保険適応がないが,4F,5Fのシースで使用できる血栓除去用のFogaty catheterが有用である(Table 2).新生児期にBASが必要となる疾患としては,心房間mixingが必要な完全大血管転位(TGA)・両大血管右室起始(DORV),生存に心房間左右短絡が必要な左心低形成症候群(HLHS)・重症大動脈弁狭窄(cAS),反対に右左短絡が必要な三尖弁閉鎖(TA)・心室中隔欠損を伴わない肺動脈閉鎖(PA IVS)などがある.
Table 2 Catheters used for BAS in Japan| Catheter | Maximum infusion volume | Maximum balloon diameter | Appropreate sheath size |
|---|
| Miller | 4 cc | 19 mm | 7F |
| Rashkind | 2 cc | 14 mm | 6F |
| Fogaty | 1.5 cc | 11 mm | 5F |
| 0.75 cc | 9 mm | 4F |
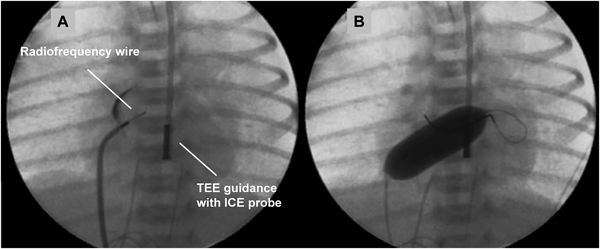
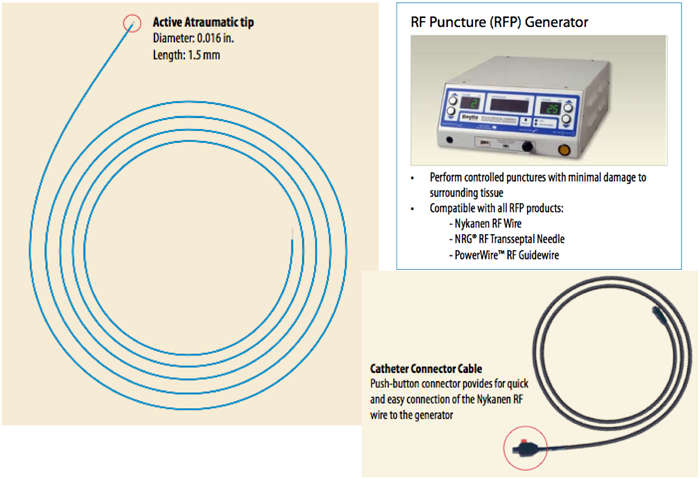
通常のBASが困難,危険,無効な状況としては,肥厚した心房中隔壁,intact atrial septum(IAS),小さいLA,低体重児,両側FVの閉塞・IVC離断などがある.肥厚した心房中隔壁に対して以前はblade atrial septostomyが施行されたが,心房壁や右室流出路(RVOT)の裂傷から死亡する合併症があり,近年はあまり施行されなくなっている2,3).これに対してballoon atrial septal dilationは効果がやや劣るが安全に施行できる.有効な欠損孔を得るためには新生児でも10~12 mm径のバルーンが必要である4,5).inflation/deflationが素早くできるArmada(12 mm×20 mm; Abot)などが適している.当院での経験になるが,Balloon atrial septal dilationにBASを組み合わせることで十分な効果が得られている.IASに対して日本では昨年までBrockenbrough needleを使用せざるを得なかった.新生児・乳児の体格でも心房中隔穿孔は不可能ではないが,特にHLHSでは心房中隔壁が厚く,それを穿孔するだけのLA容積(奥行き)がない場合が多く(Fig. 2),心房壁の穿孔・心タンポナーデの合併率が高くなる6,7).欧米では10数年前からradiofrequency wireを用いた心房中隔穿孔が施行されている(Fig. 3)8).心房中隔に接触させて通電するだけで中隔を穿孔できるので,LAが小さい新生児の肥厚したIASでもより安全に穿孔できる.日本でも2014年8月からNykanen RF wireが使用可能となった(Fig. 4).このwireの直径は0.024″,長さは265 cmで,先端のActive atraumatic tipの直径は0.016″,長さは1.5 mmである.Active tip以外の部分は整形が可能である.Connector cableでGeneratorと接続し,5~10 W,1~10 secの通電で組織の穿通が可能である.現在日本ではPA IVSの肺動脈弁穿孔とIASの心房中隔穿孔に適応があり,その使用には講習が必要である.肥厚した心房中隔のためにBASが無効の場合にはstent septostomyも有効である.留置後抗血小板薬だけでは血栓形成の報告があることから抗凝固療法が必要と思われる9).またstent migrationの報告や強度の内膜増殖を来す期間が不明であり,注意を要する10).
BASの合併症
バルーンの破裂,破裂バルーン片による塞栓,バルーンデフレーション困難,IVC閉塞・損傷,三尖弁(TV)・僧帽弁(MV)損傷,心房壁裂傷,肺静脈裂傷,高度房室ブロック・徐脈,出血などがあるが,合併症を熟知して臨むことでその多くは回避できる.近年日本で発生したBASに関連した合併症をTable 3に示す.Brockenbrough法による心タンポナーデが多いこと,近年でも心房壁等の穿孔・裂傷から死亡する症例があることを銘記すべきである.
Table 3 Complications related to BAS in reicent years in Japan| Year | Complications (number) |
|---|
| 2011 | Atrial fibrillation (1),hypotesion-death (Balloon dilation) (1) |
| 2010 | Left atrium perforation-death (1),cerebral infarction (1),stent migration-surgery (1), retroperitonear bleeding (1),atrioventricular block (1) |
| 2009 | Supraventricular tachycardia (1),pericardial effusion (2) - (Brockenbrough) (1), cardiac tamponade (Brockenbrough) (1) |
| 2008 | Tricuspid regurgitation (1),bleeding (1),stent migration-surgery (1) , internal iliac artery occlusion due to embolization of ruptured-balloon fragment (1) |
| 2007 | Atrial fibrillation (1),atrial flutter (1) |
| 2006 | Mitral regurgitation (1),tricuspid regurgitation (1), cardiac tamponade (Brockenbrough) (1) |
| 2005 | Atrial fibrillation (1),pericardial effusion (1) |
2. 新生児PA IVSに対するバルーン肺動脈弁形成術:Balloon Pulmonary Valvuloplasty(BPV)
要点
- 治療対象を厳密にすれば,右室(RV)の発育が期待できる
- カテーテル治療中最も難易度が高い手技の1つであり,重篤な合併症が起こりえる
- 術後の管理は特殊であり,重要である
- RVが発育した場合の二心室循環は良好であるが,遠隔期の問題もある
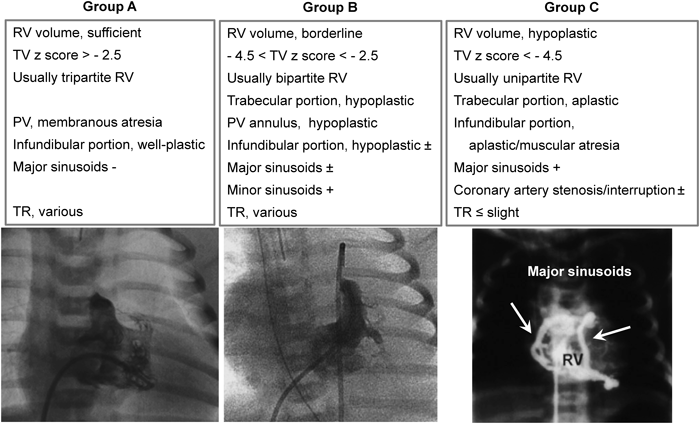
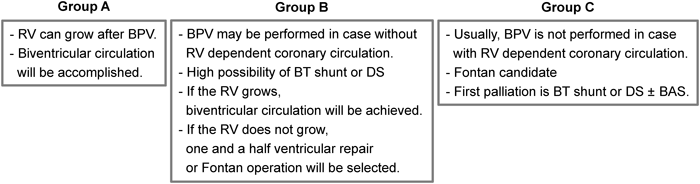
PA IVSはRVの容積と形態から3群に分類される(Figs. 5, 6).この分類はBPVの適応判断と治療後の経過の予測に有用である11).正確なRV容積は造影検査などをしないと計測できないが,TV弁輪径はRV容積と相関するので,エコー検査でもある程度の適応判定が可能である.
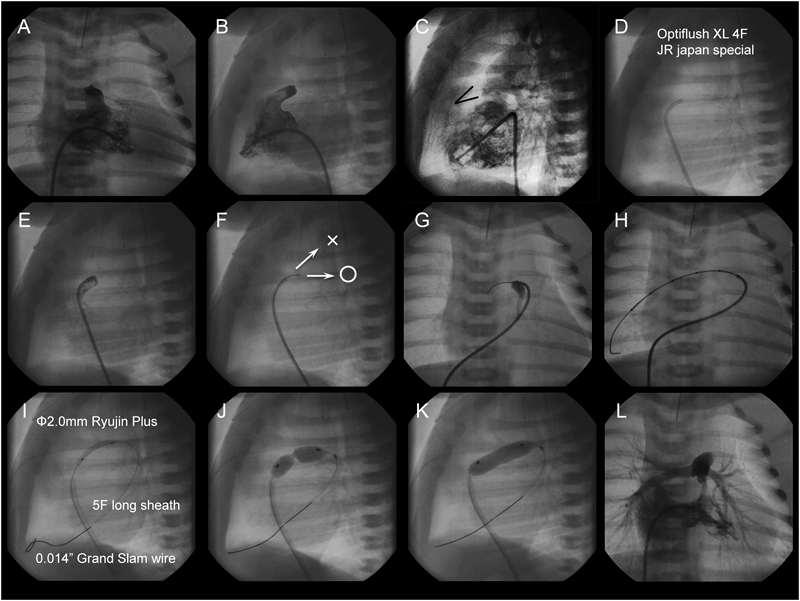
手技(Fig. 7)
- 安全に治療を遂行するためにProstagrandin E1(PGE1)の持続静注を継続するだけでなく,鎮静・筋弛緩薬を使用し,人工呼吸管理下に施行する.
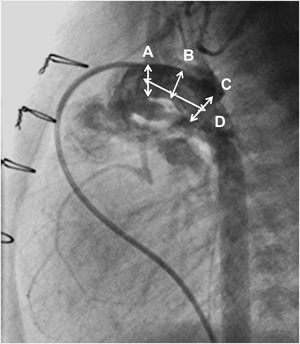
- RV造影を行い,RVの形態と容積およびSinusoidal communicationの有無を確認する(A, B).
- 左室(LV)または大動脈(Ao)造影を行い,肺動脈弁(PV)の位置を確認し,弁輪径を計測する(C).
- JR型のガイディングカテーテル(Optiflush XL 4F JR japan specialなど)を慎重にPV直下まで進める(D).
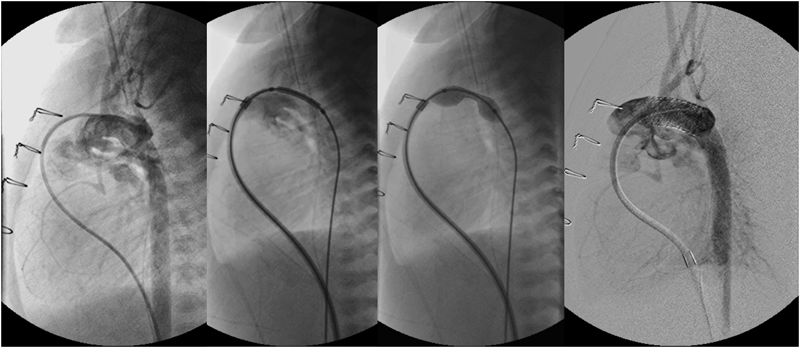
- ガイディングカテーテルの中へマイクロカテーテル(1.8F FineCrossなど)を進め,その中に先端を45°程度屈曲させた硬めの0.014″コロナリー用ガイドワイヤー(Grand Slamなど)のstiff sideを進める.JR型カテーテルはPV下の上方に位置することが多いので(E),弁穿通後上方ではなく後方へ向かう様にガイドワイヤーを整形し,RVOTの穿孔を回避する(F).正面・側面造影でガイディングカテーテルがPVに接していることを確実に把握してからガイドワイヤーを押してPVを穿孔する.その時通常は軽い抵抗を感じる.
- 弁穿孔成功後,ガイドワイヤーを肺動脈分岐部まで進めて(G),これに追従させてマイクロカテーテルを肺動脈末梢まで進める(H).あるいはガイドワイヤーをより柔らかいRadifocusなどに交換して,それを肺動脈末梢まで進めて,マイクロカテーテルを追従させる.続いてコロナリー用ガイドワイヤーのsoft sideをできる限り肺動脈末梢まで進めて留置する.
- ϕ2 mm程度のcoronary balloon catheterをPV上まで追従させて,pre-dilationを施行する.Balloon catheterが弁を通過しない場合は,弁下までLong sheathを運び,カテーテルがたわまないようにすると通過できる(I).
- 続いてPV弁輪径の120~125%の径のballoon catheterでBPVを行う(J, K).過大なballoonを選択すると将来重度の肺動脈弁閉鎖不全(PR)が生じる原因となるので注意する.
- BPVに成功すると順行性血流が増加してSpO2は上昇する.この時点では肺高血圧が残存しているので,RV圧がLV圧以下であればよい.RV造影を行い,肺動脈弁下狭窄の程度を確認する(L).弁下狭窄がなくかつRV圧がLV圧を越えている場合は1 mmサイズアップした径のballoonでre-BPVを施行する.
BPV後の管理
RVは減圧されても拡張能の改善に1~2週間要するので,1週間程度PGE1で動脈管(AD)を開存させ,酸素は使用せずに十分な鎮静と人工呼吸管理を継続する.エコーでTVの流入およびRVから肺動脈への順行性血流の増加が十分であればPGE1を中止してみる.ADが収縮してもSpO2が70%以上に維持されれば,酸素を使用して,人工呼吸から離脱する.その後RVは徐々に発育し,SpO2は上昇する.ADが収縮するとSpO2が70%以上に維持されない場合はPGE1を再開し,さらに1週間RVの拡張能が改善するのを待ってからPGE1を中止してみる.この時点でSpO2が維持できない場合は,Blalock-Taussig(BT)shuntかductal stenting(DS)が必要である.
遠隔期成績から新生児期の治療方針を考える
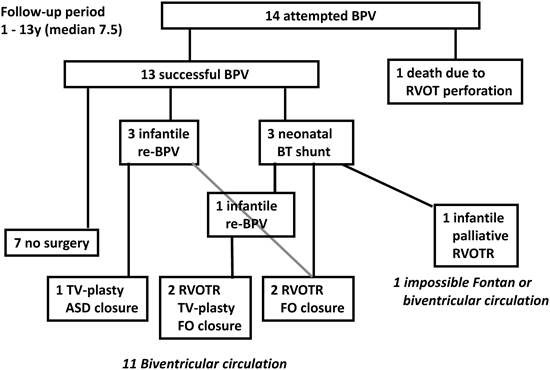
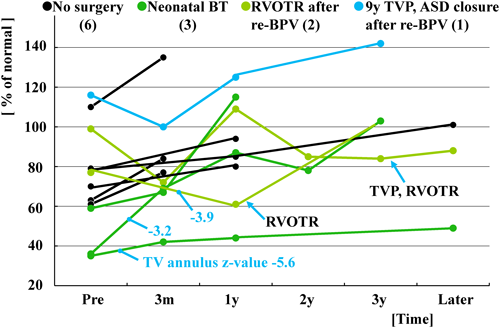
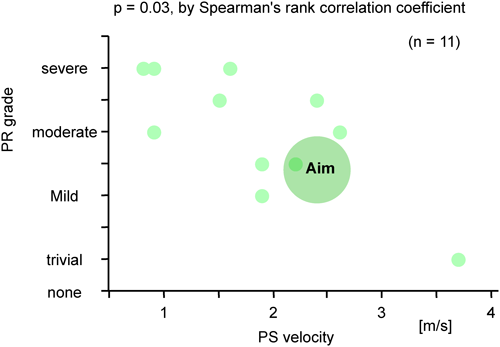
当院で1995年10月から2008年11月の間に新生児PA IVS 14症例に対して施行したBPVの遠隔成績から新生児期の治療方針を再検討した.14症例ともRV構造はtripartiteでsinusoidal communicationはない.14症例のBPV時の詳細をTable 4に示す.BPV後の経過はFig. 8にあるように13症例で手技に成功し,その内の7症例は外科治療が不要であったが,残りの6症例は経過中に新生児期のBT shuntまたは遠隔期の右室流出路形成(RVOTR)やTV-plastyなどの外科治療介入が必要であった.最終的に11症例に二心室循環が成立している.Fig. 9に示すように右室拡張末期容積(RVEDV)が40%未満ではBPVに成功しても肺血流量が不十分なために新生児期にBT shuntが必要であった.Fig. 10に示すようにBPV後RVは徐々に発育する.RVEDVが40%未満であるものが2症例あった.その内のTV弁輪径のz-valueが−4以上のものはBT shunt施行後の経過中にRVが発育した.しかしTV弁輪径のz-valueが−4未満のものはRVを通過する血流量が増加しないので,RVが発育せず,結局二心室循環が成立しなかった.一方RV圧は経過中徐々に低下してゆく(Fig. 11).Fig. 12に示すように,遠隔期に肺動脈弁狭窄(PS)の程度は徐々に軽減してゆくのに対して,PRは徐々に増加してゆく.Fig. 13に示すようにPSとPRが相反関係にあることから最終目標はPS,PRともに軽度な状態である.そのためにも新生児期のBPVで使用するballoonのサイズは可能な限りPV弁輪径の120~125%程度に留めるべきである.またPRに伴って三尖弁閉鎖不全(TR)が増悪する傾向があり,形態的に弁形成が可能であれば形成術を考慮する.これら11症例の最近の状態は心室性期外収縮以外に問題となる不整脈はなく,運動制限も疲労を感じたら休憩する程度と比較的QOLは高い.
Table 4 14 patients’ charactaristics at balloon pulmonary valvuloplasty | Range | Median | |
|---|
| Age | 1–21 | 7 | [day] |
| Weight | 2.4–3.6 | 3.2 | [kg] |
| Tricuspid valve annulus | 6.1–16.5 | 10 | [mm] |
| z-value | −5.6–3.4 | −1.5 | |
| Right ventricle (RV) end-diastolic volume | 2.6–10.6 | 5.2 | [mL] |
| % of normal | 36–161 | 63 | |
| Pulmonary valve (PV) annulus | 4–8.1 | 5.9 | [mm] |
| z-value | −5.8–0.7 | −1.9 | |
| Balloon diameter/PV diameter | 0.67–1.3 | 1.12 | |
| Note: All patients have tripartite RV and no sinusoidal communication. |
結論として適応を厳密にすれば,即ちtripartite RV, sinusiodal communicationなし,TV annulus z-score>−4, RVEDV≥60% of normal, PV annulus z-score≥−4を満たす場合に新生児期に施行するBPVの予後は良好と判断される.
3. Ductal Stenting(DS):動脈管ステント留置術
新生児期にDSが施行される場合がある疾患としてHSHS,cAS; 大動脈弓離断(IAA),大動脈縮窄(CoA);PA IVS,重症肺動脈弁狭窄(cPS);ファロー四徴(TOF),DORVなどが挙げられる.以後HLHSにおけるDSに関して述べる.BT shuntから右室肺動脈(RV-PA)conduitを用いたNorwood手術が主流となり,その成績はここ20年間に劇的に改善した12–15).しかし低体重児,右室機能低下,重度TR,IAS,染色体異常などの危険因子がある場合の死亡率は20~50%と高く,両方向性Glenn(BDG)までのinterstageの死亡もある16,17).これらのhigh risk群では高侵襲なNorwood手術を回避して,First palliationとしてより低侵襲な両側肺動脈絞扼(Bil-PAB)とDSを施行して,発育後にNorwood & BDG手術を施行することで生存率が上昇した16–18).
DSはhybrid roomでBil-PABと同時にhybridアプローチで主肺動脈にシースを挿入して留置する方法と後にカテーテル室でFVから経静脈的に留置する方法がある.ステントはself expandableとballoon expandableのものがある.経静脈的に留置する場合は合併症を起こさずに手技を遂行するための配慮が必要である.
HLHSにおける経静脈的stent留置手技
HLHSではBil-PAB後であってもカテーテルなどをRVから下行大動脈(DAo)まで進めるとRVのストレッチ,PR・TRの出現などから血圧が低下しやすいので,極力RVをストレッチさせないmaterialsを使用する.人工呼吸管理下の施行が安全だが,鎮静剤等の使用から血管拡張による血圧低下がある場合は昇圧剤を併用して血圧を高めに保つように心掛ける.
- 4F end-hole Berman catheterなどで主肺動脈造影を行い,ADを描出し,その径(肺動脈側,再狹部,大動脈側)と全長を計測する(Fig. 14).将来のNorwood手術を考慮するとAD全長が過不足なく覆われるDSが理想的で,stent径はmigrationを避けるために参照血管径+1~2 mmのものを選択する.
- 通常のstent留置方法(back loading法;Fig. 15) ガイドワイヤーはADの形状に合致するように逆U時状に整形して用いる.Long sheathをDAoまで進めて,その中を通してstentをADまでdeliveryする.Sheathを引いてstentを露出し,sheathから確認造影をしてstent位置を調節して,stentを留置する.
- Bare delivery technique(Fig. 16) 血圧が低下するためにLong sheathをDAoへ運べない場合に有用である.Long sheathは用いないか,RVまで進めておく.ガイドワイヤーはADの形状に合致するように逆U時状に整形する(B; 矢印).stentをBareの状態でADまでdeliveryする(C).Delivery時に血圧が低下する場合は10倍希釈エピネフリン(5~10 µg)をsheathから静注する(通常血圧は20~30 mmHg程度上昇する).血圧が維持されている間に,気管チューブや胃チューブを位置決めの対象としてstentを留置する(D).ADの狭窄部が限局している場合はstent migrationが生じやすいので,可能な限り最狹部にステント中央部が位置するように留置する.
合併症・問題点
2006年10月から2013年10月の間に当院で12症例(Table 5)に施行したDSの最中または後に生じた合併症・問題点をTable 6に示す.最多の問題は手技中の血圧低下であり,12症例中7症例に認められ,その内の5症例はHLHSであった.特に大動脈弁閉鎖では血圧低下から冠血流が低下して重篤な心機能低下をきたし得るので,Bare stent deliveryやエピネフリン静注などの対応を施して手技に臨む必要がある.
Table 5 Characteristics of 12 cases receiving DS at our hospital| Age (day) | 3–107 (median 24) |
| Weight (kg) | 2.0–3.3 (median 2.7) |
| Underlying disaese | HLHS (6), cAS (2), unbacanced AVSD (1), IAA (2), TA TGA (1) |
| Length of AD (mm) | 4.3–32.7 (median 17.0) |
| Diametr of AD (mm) | |
| Pulmonary arterty side | 2.7–9.4 (median 6.3) |
| Center | 1.9–7.9 (median 3.9) |
| Ao side | 3.8–10.5 (median 6.9) |
| Stent *before remount | |
| Size | Medium (5), Small (9) |
| Diameter (mm) | 5–10 (median 6) |
| Length (mm) | 12–29 (median 18) |
| Way of implantation | Common (5), Bare delivery (6), Hybrid (1) |
| Stent afer implantation | |
| Diameter (mm) | 4.9–9.7 (median 8.0) |
| Length (mm) | 9.8–18.3 (median 15.5) |
| DS, ductal stenting; HLHS, hypoplastic left heart syndrome; cAS, critical aortic valve stenosis; AVSD, atrioventricular septal defect; IAA, interrupted aortic arch; TA, tricuspid atresia; TGA, transposition of the great arteries; AD, arterial duct. |
Table 6 The ways to deal with problems and complications accompanied with DS in the 12 cases| Problems/complications | n | How to deal with it |
|---|
| Decrease of blood pressure during the procedure | 7 | Forming the guide wire into an invert U shape |
| Bare stent delivery |
| Injection of epinephrin (5–10 µg) |
| Ductal constricriction of the part where is not covered the previous stent | 2 | Additional stenting |
| Fear to compress the bronchus because of right DAo and a long course of the AD | 1 | Covering only the narrow part of pulmonary artery side in the AD |
| Alternative way: use of selfexpandable stent |
| Dissection of DAo | 1 | Additional stenting |
| Development of CoA | 1 | Norwood procedure |
| Need for the catheter to turn in the LV to delivery | 1 | Delivery from FA |
| DS, ductal stenting; DAo, descending aorta; CoA, Coarctation of the Aorta; LV, left ventricle; FA, femoral artery. |