先天性横隔膜ヘルニア(CDH)では発生の比較的初期の横隔膜形成不全により腹部内臓(肝臓,胃,腸)が胸腔内に入り成長するため肺と心臓が低形成になり,手術成績が不良となる1–3).その胎生期肺低形成の臨床診断は超音波とMRIによる4, 5).現在周産期医療において救命困難な本症重症例に対する胎児診断からの治療戦略が模索されている.
ラット胎仔の全身急速凍結法による凍結標本を凍結ミクロトームで切り,その断面の心臓大血管像(写真)から種々の計測を行う方法は50年前に動脈管の研究用にKarolinska研究所で開発され6),40年前から私も用いてきた7, 8).催奇形薬bis-diamineは妊娠ラットに大量投与するとその胎仔の40%に横隔膜ヘルニアを生じるので,私は横隔膜ヘルニアの肺と心臓の低形成を論文9)にした.その研究のカラー写真は未発表なのでここに図譜として提示する.これらの横隔膜ヘルニアの心臓肺断面カラー写真から肺低形成と心臓低形成が明瞭に理解される.
ラット満期胎仔の全身急速凍結法による実験7–9)を次のように行った.ラットの妊娠期間は21.5日なので,妊娠21日目に親ラットを頸椎脱臼法で安楽死させ,ただちに帝王切開で取り出した胎仔を胎盤つきのままドライアイス–アセトン(−76°C)に投入して瞬時に凍結する.凍結した胸部横断面(transverse)を凍結ミクロトームで切り,断面を0.5 mm毎に実体顕微鏡(Wild 400)で撮影する.1個体の胸部から約20断面を同じ倍率で撮影する.
Bis-diamineによる先天性心疾患と横隔膜ヘルニア8–10)は次のように作製した.妊娠9日目と10日目にWistarラット40匹にbis-diamine 200 mgを胃内注入し,妊娠21日に合計300匹の胎仔を調べると,90%の胎仔に心疾患8, 9)が認められた.更に胸腺の無-低形成(100%),横隔膜ヘルニア(40%,120例:左100,右20)の合併があった.
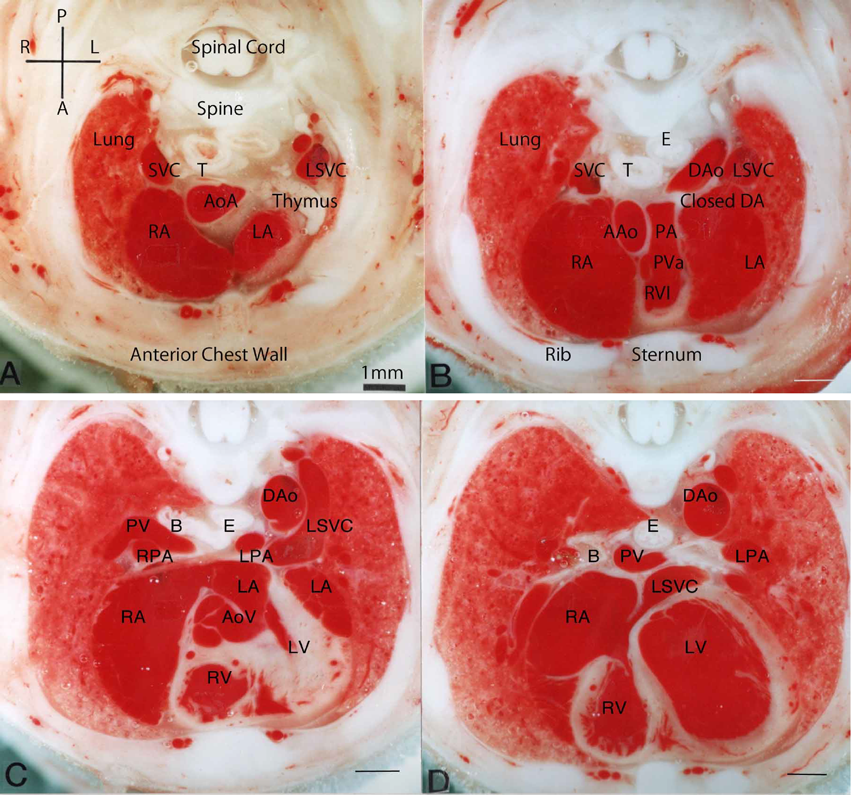
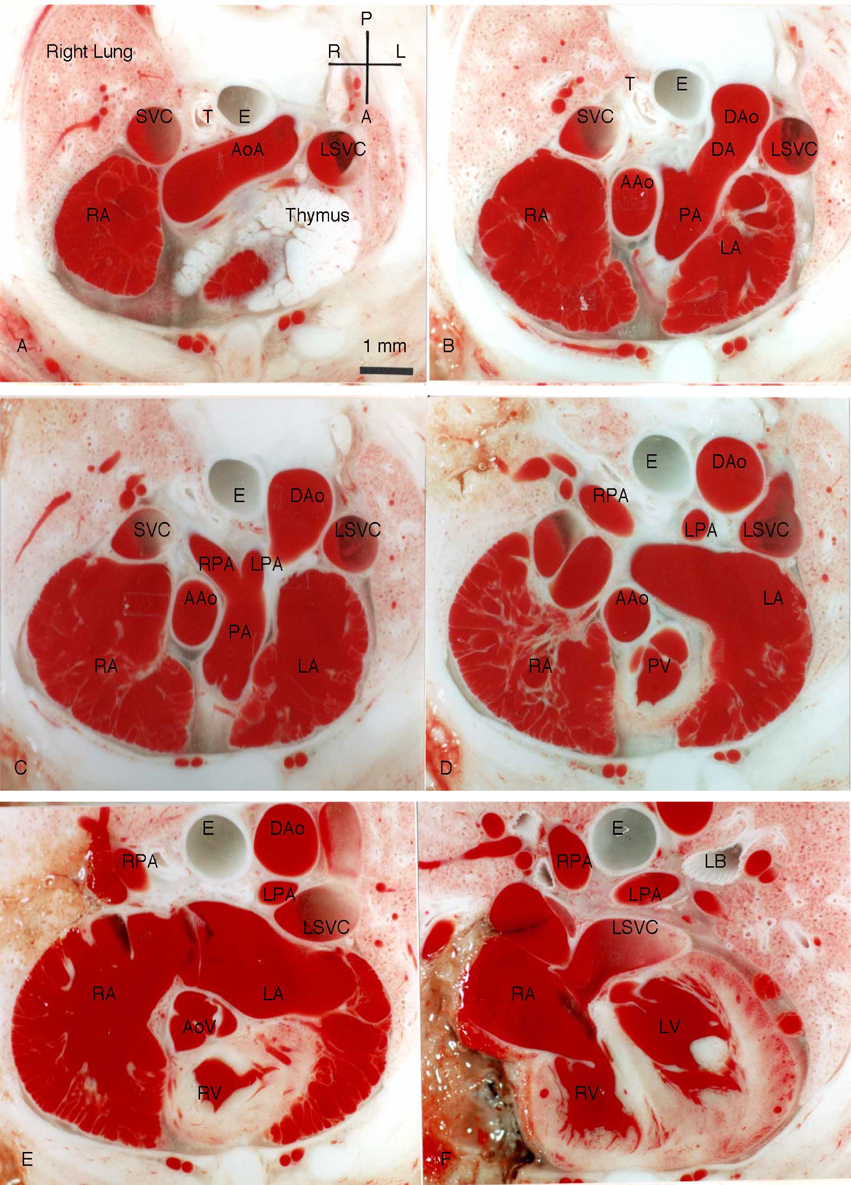
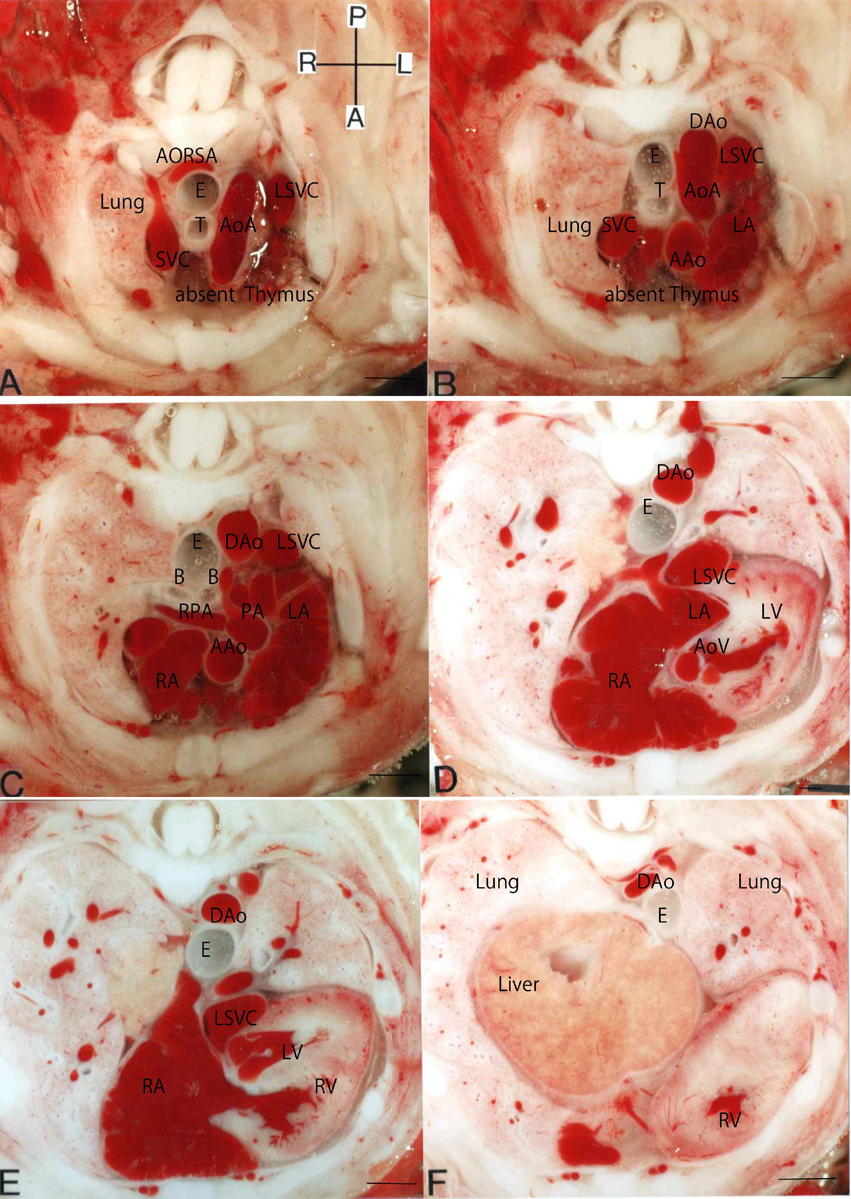
Fig. 1, 2に正常ラット新生仔と胎仔の横断面を示す.ヒトで左上大静脈は胎生初期にのみ生じるが,げっ歯類,ラットでは生後まで存続する11).Fig. 1の新生仔では胎仔と異なり,肺は鮮紅色で容積が大きく,食道は扁平であり,動脈管は閉じて索状である.右室と左室は大きい.
Fig. 2の正常胎仔では新生仔と比べて胸腺が大きく,動脈管が太く,肺動脈と肺静脈が細い.ラット胎仔の食道はヒト胎児と異なり常に太く開いている.房室弁と半月弁は大部分で半ば開いている.
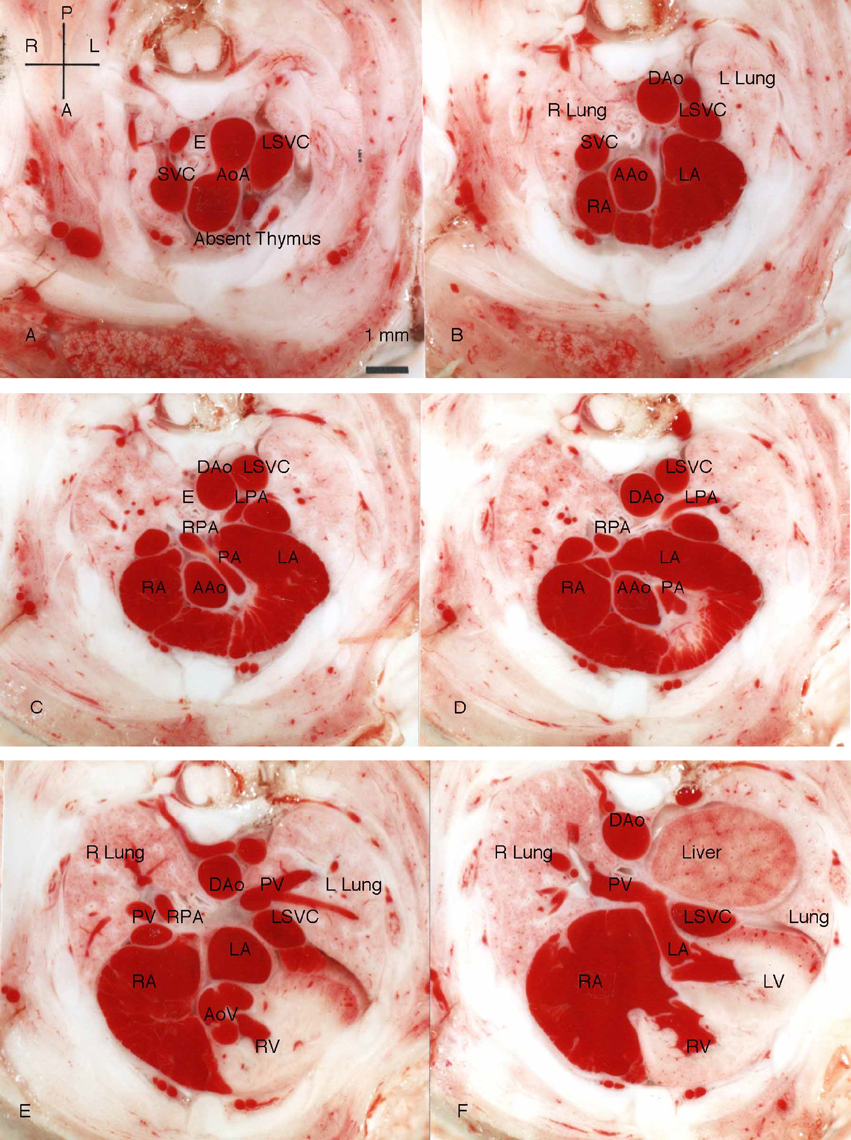
Fig. 3以下にbis-diamine投与後ラット胎仔例を示す.Fig. 3は心臓と横隔膜が正常の例である.胸腺は欠損しているが,肺と心臓の大きさは正常である.
Fig. 4は軽度の左横隔膜ヘルニア,Fallot四徴症と胸腺欠損の例である.肝臓の一部が左胸郭後部に入り,左肺がやや小さいが,心臓と縦隔は偏位なく,右肺と心臓の大きさは正常である.
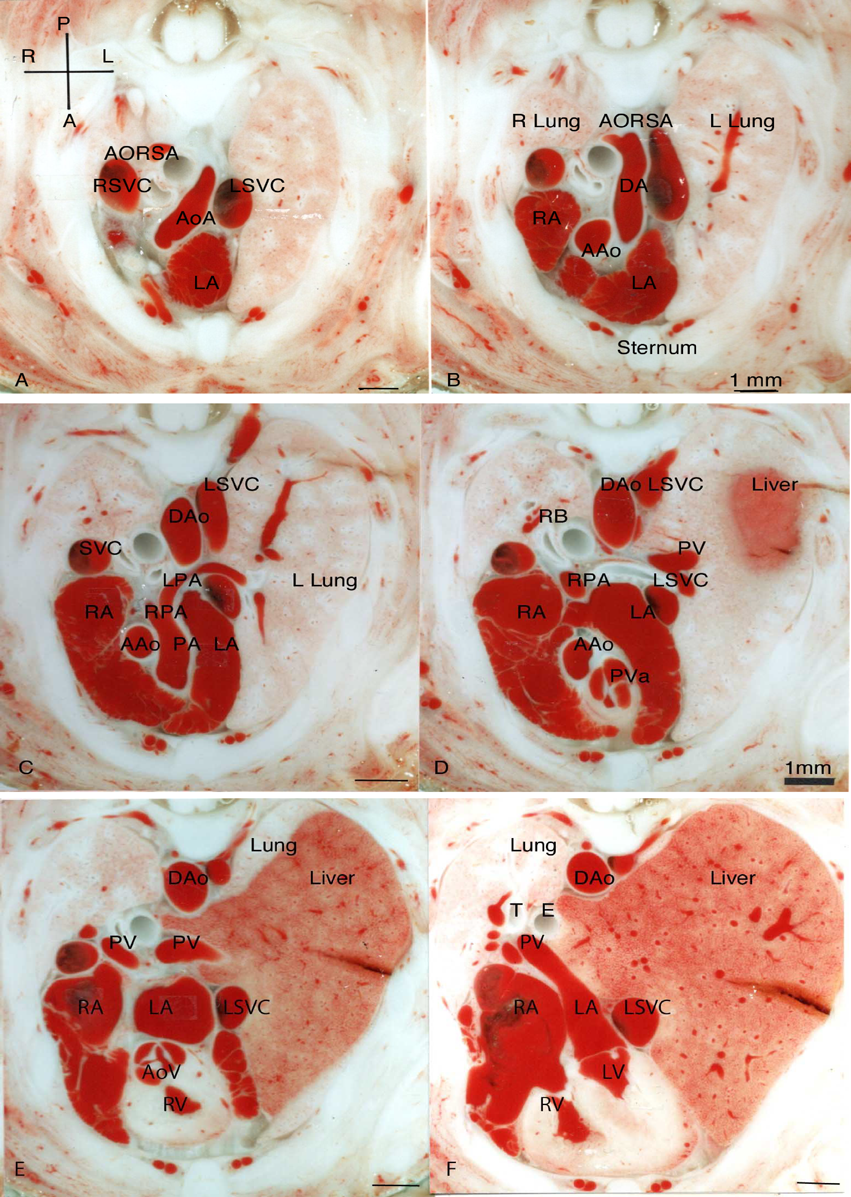
Fig. 5は胸腺欠損,右鎖骨下動脈起始異常,中等度左横隔膜ヘルニア,中等度肺低形成,心臓低形成の例である.左胸郭に入り込んだ肝臓により,心臓と縦隔が右に圧排されている.
Fig. 6は高度の左横隔膜ヘルニア,総動脈幹残遺,胸腺欠損,高度な肺低形成の例である.ヘルニア孔から肝臓と胃が胸腔に入り,肝臓が左胸隔すべてを占拠して左肺は肺尖部に痕跡的に存在する.肝臓は更に縦隔を超えて右胸郭内まで入り,右肺の低形成を生じている.心臓は右に偏位して小さい.
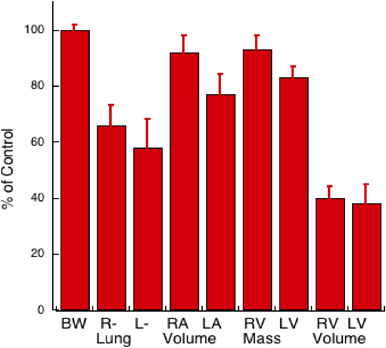
Fig. 7に心奇形を合併しない左ヘルニア11例の体重,肺容積,心房心室容積,心室筋量を対Control %値で示す.ControlはFig. 3の例を含む心臓横隔膜正常の10例である.
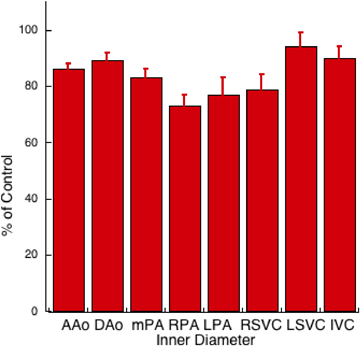
Fig. 8に心奇形を合併しない左ヘルニア11例の大動脈,肺動脈,大静脈の内径を対Control %値で示す.
Fig. 9は右横隔膜ヘルニア,右鎖骨下動脈起始異常,肺と心臓の低形成の例である.肝臓の一部が右胸郭後部に入り,心臓が左に圧排されて内腔が小さくなり,左右肺も小さい.
ここに示したラット横隔膜ヘルニアではヒトの小腸と結腸がまず胸郭内に脱出する臨床例と異なり肝臓が主に脱出していた.その理由はラットでは肝臓が横隔膜の腹腔面全面で厚い円盤状で張り付いているため,ヘルニア孔からまず肝臓だけが胸郭内に脱出するためである.正常ラットの食道は横隔膜と厚い肝臓を通過して腹腔に入って胃に移行する.ヘルニアでは胎生期に胸腔を占拠した腹部臓器は肺と心臓を圧迫してその成長を抑えて低形成を生じるが,その作用は内腔臓器である小腸や大腸よりも実質臓器である肝臓のほうが強いと推定される.bis-diamine投与後のラット胎仔横隔膜ヘルニアではヘルニアの大小にかかわらず胸郭の大きさは同じなので,胸腔内を占拠した肝臓と胃の量に比例して肺と心臓(両心室)の低形成が生じている.心室の低形成はFig. 7に示す如く心筋量の軽度減少,容積の高度減少であり,拡張障害を示し,胸腔内腹部臓器による圧迫によると考えられるが,組織学的検索ではbis-diamineでラット胎仔心筋構造異常10)も報告されているので,病的肥大の関与の可能性もある.
ヒト横隔膜ヘルニアでは通常右室は正常で左室が低形成になるのと異なり,ラットではここに示したように左右両心室の低形成を生じていた.ヒトのヘルニアでは左室低形成の機序として,1. 肺低形成による肺–左房左室への血流低下,2. 胸腔を占拠した腹部臓器による圧迫,3. 心臓の右への偏位による下大静脈血の卵円孔経由の左房流入減少の3機序12)が推定されているが,ラットでは2が主に作用したことになる.
臨床上ヘルニア手術後の致死因子としては肺低形成による肺血管床減少,肺高血圧が主であるが,心臓低形成の関与も推定される.先天性横隔膜ヘルニア重症例の胎児治療には気管閉塞術13)が始まり,薬物治療14, 15)が模索されている.Inamura16)は胎児診断例の重症度に関連した出生後薬物療法を論じている.本症の肺高血圧の成因は従来肺低形成によると考えられてきたが,最近先天性横隔膜ヘルニア形成因子であるPBX17)が出生時肺血管拡張因子18)と判明し,この因子の欠如も肺高血圧に関与すると推定される.
横隔膜ヘルニアの12%に先天性心疾患が合併19)し,ファロー四徴症の合併2)も報告されている.最近22q11.2欠失症候群の0.8%に横隔膜ヘルニアが合併することが報告20)された.したがってこの図譜のFigs. 4~6の如く,臨床胎児エコーで先天性心疾患,conotruncal anomalyと横隔膜ヘルニアの合併する例は22q11.2欠失症候群の可能性が高い.
引用文献References
1) Yamoto M, Inamura N, Terui K, et al: Echocardiographic predictors of poor prognosis in congenital diaphragmatic hernia. J Pediatr Surg 2016; 51: 1926–1930
2) Kotecha S, Barbato A, Bush A, et al: Congenital diaphragmatic hernia. Eur Respir J 2012; 39: 820–829
3) Chandrasekharan PK, Rawat M, Madappa R, et al: Congenital diaphragmatic hernia: A review. Matern Health Neonatol Perinatol 2017; 3: 6
4) Victoria T, Danzer E, Adzick NS: Use of ultrasound and MRI for evaluation of lung volumes in fetuses with isolated congenital diaphragmatic hernia. Semin Pediatr Surg 2013; 22: 30–36
5) Claus F, Sandaite I, Dekoninck P, et al: Prenatal anatomical imaging in fetuses with congenital diaphragmatic hernia. Fetal Diagn Ther 2011; 29: 88–100
6) Hörnblad PY, Larsson KS: Studies on closure of the ductus arteriosus 1: Whole-body freezing as improvement of fixation proceedures. Cardiologia 1967; 51: 231–241
7) 門間和夫:動脈管薬の実験40年.日小児循環器会誌2016; 32: 261–269
8) Momma K, Ando M, Takao A: Fetal cardia morphology of tetralogy of Fallot with absent pulmonary valve in the rat. Circulation 1990; 82: 1343–1351
9) Momma K, Ando M, Mori Y, et al: Hypoplasia of the lung and heart in the fetal rat with diaphragmatic hernia. Fetal Diagn Ther 1992; 7: 46–52
10) Kuribayashi T, Roberts WC: Tetralogy of Fallot, truncus arteriosus, abnormal myocardial architecture and anomalies of the aortic arch system induced by bis-diamine in rat fetuses. J Am Coll Cardiol 1993; 21: 768–776
11) Hebel R, Stromberg MW: Anatomy and Embryology of the Laboratory Rat. Wörthsee, BioMed Verlag, 1986, pp112–113
12) 矢本真也,福本弘二,宮野 剛,ほか:胎児心臓超音波検査による先天性横隔膜ヘルニアの新しい重症度指標.日小外会誌2015; 51: 205–2120
13) Mous DS, Kool HM, Wijnen R, et al: Pulmonary vascular development in congenital diaphragmatic hernia. Eur Respir Rev 2018; 27: 170104
14) Luong C, Rey-Perra J, Vadivel A, et al: Antenatal sildenafil treatment attenuates pulmonary hypertension in experimental congenital diaphragmatic hernia. Circulation 2011; 123: 2120–2131
15) Umeda S, Miyagawa S, Hukushima S, et al: Enhanced pulmonary vascular and alveolar development via prenatal administration of a slow-release synthetic prostacyclin agonist in rat fetal lung hypoplasia. Pros One 2016; DOI: 10.137/journal.pone.01611334
16) Inamura N, Kubota A, Nakajima T, et al: A proposal of new therapeutic strategy for antenatally diagnosed congenital diaphragmatic hernia. J Pediatr Surg 2005; 40: 1315–1319
17) Russell MK, Longoni M, Wells J, et al: Congenital diaphragmatic hernia candidate genes derived from embryonic transcriptomes. Proc Natl Acad Sci USA 2012; 109: 2978–2983
18) McCulley DJ, Wienhold MD, Hines EA, et al: PBX transcription factors drive pulmonary vascular adaptation to birth. J Clin Invest 2018; 128: 655–667
19) Takahashi S, Sago H, Kanamori Y, et al: Prognostic factors of congenital diaphragmatic hernia accompanied by cardiovascular malformation. Pediatr Int 2013; 55: 492–497
20) Unolt M, DiCairano L, Schlechtweg K, et al: Congenital diaphragmatic hernia in 22q11.2 deletion syndrome. Am J Med Genet 2017; 17: 135–142