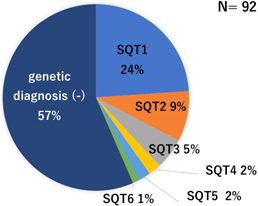
SQTSは心電図でのQT短縮が特徴の致死的不整脈である.2000年に初めて報告され3),現在までに約100例の症例報告がある.心臓の形態異常は伴わない.原因としてイオンチャネル遺伝子異常が知られ,6種類の責任遺伝子が報告されているが4)(Fig.1),遺伝子異常が同定されない症例が半数以上ある(Fig. 2).心室頻拍や心室細動,心房細動が惹起され,失神や若年突然死の原因となる.臨床像はまだ不明な点が多い.
1. SQTSの病態生理
イオンチャネル異常により,内向きカルシウム電流の減弱や外向きカリウム電流の増強が起こり,再分極が早まる.心筋細胞レベルでは活動電位は短縮し,心電図上ではQT間隔が短縮する(Fig. 1).不均一な再分極に伴うphase 2 reentryが心室細動や心室頻拍の引き金と考えられ,QT延長症候群に似る5).
2. SQTSの診断
1)診断基準
2011年にGollobらが初めてSQTSの診断基準を提唱した6).QT延長症候群のSchwartzスコアのようにスコア化されている.QT間隔に加え,Jpoint-Tpeak間隔,既往歴,家族歴,遺伝子検査の所見を加味し,診断する(Table 1).その後,診断基準は2013年に3大陸合同のExpert consensus statementで発表され1)(Table 2),2015年に欧州心臓病学会のガイドラインで示された2)(Table 3).この2つではQT短縮所見のみでもSQTSと診断しうる.Expert consensus statementではQTc≦330 ms,欧州心臓病学会ではQTc≦340 msがSQTSとなる.この点以外は2つの診断基準はほぼ同じである.いずれの診断基準でもBazettの心拍補正を用いている.
Table 1 SQTS diagnostic criteria presented by Gollob et al.6) | Point |
|---|
| QTc (Bazett) ms | |
| <370 | 1 |
| <350 | 2 |
| <330 | 3 |
| Jpoint-Tpeak interval<120 ms | 1 |
| Clinical history | |
| History of sudden cardiac arrest | 2 |
| Documented polymorphic VT or VF | 2 |
| Unexplained syncope | 1 |
| Atrial fibrillation | 1 |
| Family history | |
| 1st or 2nd -degree relative with high-probability SQTS | 2 |
| 1st or 2nd -degree relative with autopsy-negative SCD | 1 |
| SIDS | 1 |
| Genotype | |
| Genotype positive | 2 |
| Mutation of undetermined significance in a culprit gene | 1 |
| High-probability SQTS: ≥4 points, intermediate-probability SQTS: 3 points, low-probability SQTS: ≤2 points. Electrocardiogram: must be recorded in the absence of modifiers known to shorten the QT interval. J point-T peak interval must be measured in the precordial lead with the greatest amplitude T-wave. Clinical history: events must occur in the absence of an identifiable etiology, including structural heart disease. Points can only be received for 1 of cardiac arrest, documented. polymorphic VT, or unexplained syncope. Family history: points can only be received once in this section. * A minimum of 1 point must be obtained in the electrocardiographic section in order to obtain additional points. VF; ventricular fibrillation, VT; ventricular tachycardia |
Table 2 Expert consensus recommendations on SQTS diagnosis1)| SQTS is diagnosed; |
| QTc (Bazett)≦330 ms |
| SQTS can be diagnosed; |
| QTc (Bazett)<360 ms |
| and one or more of the following: |
| ① a pathogenic mutation |
| ② family history of SQTS |
| ③ family history of sudden death at age ≤40 years |
| ④ survival of a VT/VF episode in the absence of heart disease |
| Red font indicates differences from the European Society of Cardiology guideline (Table 3). |
Table 3 Diagnosis of SQTS according to the European Society of Cardiology guideline2)| SQTS is diagnosed; |
| QTc (Bazett)≦340 ms |
| SQTS should be diagnosed; |
| QTc (Bazett)≦360 ms |
| and one or more of the following: |
| ① a confirmed pathogenic mutation |
| ② family history of SQTS |
| ③ family history of sudden death at age<40 years |
| ④ survival of a VT/VF episode in the absence of heart disease |
| Red font indicates differences from expert consensus recommendations (Table 2). |
2)診断時の注意点
診断にはいくつかの注意点がある.まず2次性のQT短縮を除外しなければならない.様々な原因でQT短縮が起こる7)(Table 4).
Table 4 Secondary causes of short QT interval| Hyperkalemia |
| Hypercalcemia |
| Hyperthermia |
| Acidosis |
| Effect of catecholamine |
| Activation of I K Ach |
| Activation of I K ATP |
| Effects of drugs such of digitalis |
| Carnitine deficiency |
| Modified based on reference 7. |
QT間隔の測定法や心拍補正法によりQTcは異なる8).Bazett補正では徐脈時はQT間隔を過剰補正してSQTSを過剰診断,頻脈時にはQT間隔を過小補正してSQTSを過小診断する懸念がある.一方Fridericia補正では頻脈時に過剰診断する懸念がある.また頻脈時には正常者とQT間隔がoverlapする可能性ある9).このために心拍数60/分前後での評価が推奨されている.しかし小児では心拍数60/分前後での心電図測定が困難なことが多いのが問題である.
さらに洞機能不全例での評価には注意を要する.洞機能不全があると交感神経刺激によりQT間隔が短縮しても,心拍数上昇(RR間隔短縮)が伴わないためQTcが短縮する可能性がある10).
3. SQTS既報例の臨床像
過去のSQTS患者についての報告で,1)有症状,2)SQTSまたは若年突然死の家族歴,3)遺伝子診断確定,のうち少なくとも一つを満す既報例を対象として,臨床像をまとめた4, 6, 11–24).対象患者は92例だった.Bazett補正QTcは194~377 msであった.うちQTc>360の2例は遺伝子診断され,突然死の家族歴があった6).それ以外の症例は3大陸合同のExpert consensus statementの診断基準を満たしていた.約6割が遺伝子型不明であった(Fig. 2).
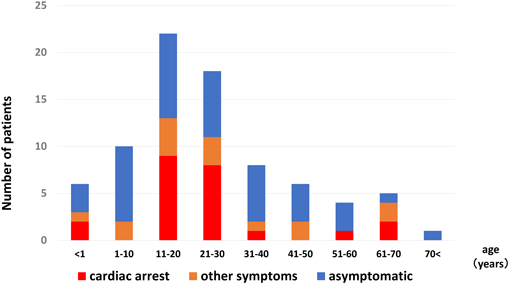
男性が多く,男女比は7 : 3であった.診断時年齢は0~80歳と幅広いが,30歳以下の若年者が3分2以上を占めた(Fig. 3).心停止例は92例中25例(27%)で,うち30歳以下が8割以上を占め,若年者がほとんどであった(Fig. 3).発症年齢に性差があった(Fig. 4).男性では10~20歳代での発症が殆どだが,女性では発症年齢の偏りはなかった.思春期以降の男性に発症する点はBrugada症候群に似ており,男性ホルモンの影響が推察される.しかし発症年齢は30~40歳代が多いBrugada症候群に比しSQTSは少し若い.その明確な理由はわからないが,これはBrugada症候群と比べ加齢の影響が少ないのかもしれない.
心房細動は17例(18.5%)に,洞機能不全は7例(7.6%)に合併していた.心房細動はSQT1−4に報告があった.一方,洞機能不全合併7例中6例は胎児期徐脈を契機に診断されたSQT2,KCNQ1-V141M変異例であった.この変異は胎児新生児期の徐脈と若年発症心房細動が主体である点,QT短縮を伴わない洞機能不全例や心電図異常を認めない例もあり,型に幅がある点など,他のSQTSとは臨床像が異なった.
無症状例は47例(51%)であった.
4. 検査
1)12誘導心電図
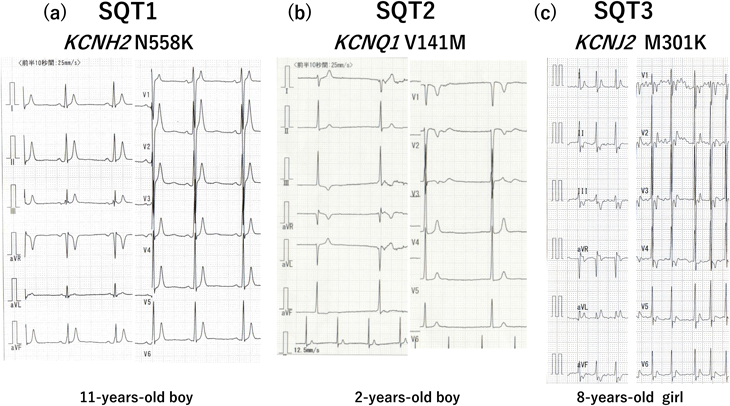
診断に最も重要である.QT間隔を評価するだけでなく,T波形も重要な所見である.T波形は遺伝子型で異なることが知られている(Fig. 5).SQT1では高く左右対称性なT波形が多い.最も報告の多いKCNH2-N588K変異13, 25)や他の変異でも報告されている12).SQT2は様々である.最も報告の多いKCNQ1-V141MのT波は高くないが24),高いT波を示す他の変異の報告もある14).SQT3では左右非対称なT波の報告が多い.T波が急峻に立ち上がる例と17),逆にTpeakから急峻に下降する例がある6).SQT4-5はBrugada型心電図を示す23).QT短縮の程度と重症度の関連は示されていない.12誘導ECGの所見によるリスク層別化の試みは後述する.
2)運動負荷試験・ホルター心電図
運動負荷試験やホルター心電図においてはQT間隔が短縮し,正常に比し心拍数の変化に伴うQT間隔の変化が乏しいのが特徴である9).ホルター心電図は心房細動の合併評価にも有用である.
3)電気生理学検査
心室細動や心室頻拍の誘発頻度は低いが,心室不応期は短い.正常群と比較した検討では,右室流出路の不応期200 ms未満を基準とすると感度86%,特異度100%と報告がある26).
5. 生活管理と治療
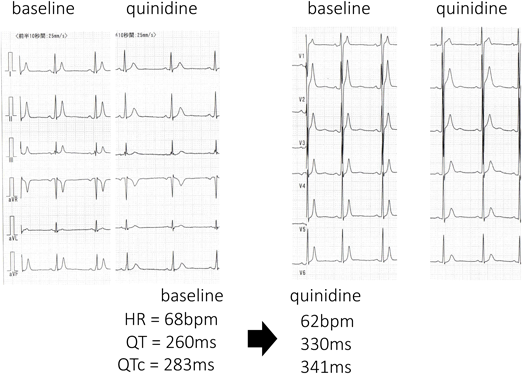
生活管理や治療に関するエビデンスは乏しく,運動制限の有効性は示されていない.薬物治療も十分と言えるエビデンスはないが,キニジンの有効性が報告されている.特にSQT1でQT間隔が正常化する例があり心イベント抑制効果が期待される25, 27)(Fig. 6).ソタロールなどのIII群薬はSQT1に対するQT延長効果は乏しいが,他のサブタイプで効果が期待されている.Expert consensus statement1)や欧州心臓病学会のガイドライン2)では,「突然死の家族歴のある無症状例に対してキニジンやソタロール投与を考慮しても良いかもしれない」としている(class IIb).
ICDが突然死防止に有用と言えるが,QTが極端に短縮しているため,T波をQRSと認識し誤作動する場合がある.Expert consensus statement1)と欧州心臓病学会2)のガイドラインではICD植え込みを,1)心停止既往例,2)持続性心室頻拍の既往者(意識の有無にかかわらず)に推奨している(class I).さらに突然死の家族歴のある無症状例については,Expert consensus statement1)では考慮してもよいかもしれないとし(class IIb),欧州心臓病学会のガイドライン2)では個々の症例での判断を勧めている.
これまで様々な集団からQT短縮例を抽出した報告がある8, 10, 28–34).このなかにはSQTSの診断基準を満たす症例も含まれていおり,SQTSの頻度や臨床像を知ることにもつながる.
報告によりQT短縮例の頻度は異なり,QT間隔の測定方法の違いに加え,母集団の違いが頻度に影響していると推察される.成人の報告では人種,性別,年齢により頻度が異なると指摘している.男性,黒人にQT短縮例が多く,性ホルモン(テストステロン)の影響が推察されている33).病院受診例を対象とした報告では,男女共に10~20歳代にかけてQT短縮例が多かったが,その理由は不明である32).さらに競技スポーツ者にQT短縮例が多かったという報告があり,運動による再分極の変化が推察されている33).また成人QT短縮例の長期予後は良好と報告されている28, 29, 33).
小児の報告はわずかであるが,シンシナティ小児病院の心電図データベースを基にした報告がある34).21歳未満の心電図272,504件を対象としてBazett補正でQTc<340 msを抽出基準とし,45例(0.05%)が抽出された.平均10.7か月フォローし,2例が死亡したがいずれも不整脈死ではなかった.
一方,我々は一般小児のQT短縮の頻度を知るため,新潟市学校心臓検診の小学校1年生(小1)6,607名と中学校1年生(中1)6,707名を対象として研究を行った.QTc<330 msを抽出基準とした.抽出例数は,Bazett補正で小1は男1名(0.01%)のみ,中1は13名(0.2%,男9名)であった.またFridericia補正では小1は20名(0.3%,男7名),中1は11名(0.16%,男6名)であった.我々の一般小児集団が米国小児病院受診者集団より低い抽出基準であったのにもかかわらずQT短縮例が高頻度であった.どちらの報告にも有症状のSQTS例はなかった.
以上より,様々な集団から抽出されるSQTSのほとんどが無症状のようである.
SQTSのなかでも,高リスクの既報例と検診・健診などで抽出される低リスク例には臨床像に大きな隔たりがあり,高リスク例の鑑別が重要である.これまでにも12誘導心電図で鑑別を試みた報告がいくつかある.AnttonenらはJpoint-Tpeak間隔を鑑別の指標として報告している35).彼らは心停止や心室頻拍の既往のある高リスクの10例(うちSQT1が4例)と集団より抽出された無症状のSQTS12例を比較した.Jpoint-Tpeak間隔は高リスク群が有意に短く,2群の値が重ならなかった.しかし検診・健診では,Jpoint-Tpeak間隔を新たに測定する必要がある.
Watanabeらは早期再分極を鑑別の指標として報告している36).彼らは,心停止,心室頻拍,失神の既往のある高リスクの25例と,SQTSの家族歴や遺伝子診断があるが無症状の低リスクの12例を比較した.高リスク例では22例(88%)に早期再分極を認め,一方無症状例では2例(17%)であり,早期再分極は,両者の鑑別に役立つとした.しかし集団から抽出された家族歴も遺伝子診断もない無症状のSQTSでも30%に早期再分極を認め,検診・健診での高リスク例抽出には向かない.
TulumenらはPQ部分の深さを指標として報告している37).基線から0.05 mV以上深いPQ部分をPQ低下と定義し,無症状例も含めたSQTS64例と対象群を比較した.SQTS群では81%にPQ低下を認めたが,対照群では21%であり,頻度に有意差を認めた.さらに心房細動を合併した6例全例にPQ低下を認めた.しかし心停止・失神症既往のSQTS例とその他のSQTS例とに差はなかった.またPQ波の深さ計測は簡便さに欠け,検診・健診での高リスクSQTS例抽出には向かない.
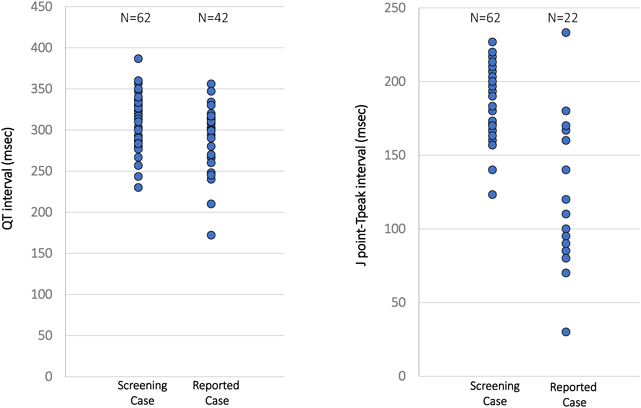
そこで我々は,既報の有症状SQTS症例と,学校心臓検診で抽出された無症状のQT短縮者の心電図所見を比較検討した.既報のSQTSはQTcと心拍数が確認できた症例42例を対象とした.学校心臓検診群では,自動診断のBazett補正またはFridericia補正がQTc<360 msとなった小1と中1の62例を対象とした.さらにJpoint-Tpeak時間も確認できた例はこれも検討した.またQT時間は接線法で再測定した値を採用した.
QT時間やQTcでは両群の重なりが多く(Fig. 7, 8),鑑別の指標には適さなかったが,Jpoint–Tpeak<120 mは検診群になく,この指標の特異度は高いと考えられた(Fig. 8).しかしSQTSではTpeakが遅い例もあり,感度は低い.