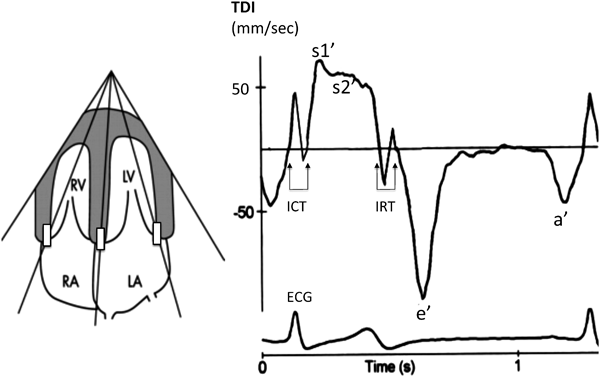
TDIにて任意の心筋部位にサンプルボリュームを設定すれば,その部位の組織ドプラ波形をスペクトル表示することができる.ここでは心尖部四腔断面から僧帽弁輪(外側)での心筋運動速度波形の解析について説明する.
左室心筋は心外膜側と心内膜側の斜走筋,中間層の輪状筋の3層構造を呈する.左室短軸断面での左室内径短縮率は主に輪状筋の機能を評価している.一方,多くの心筋病変では心内膜下に病変が出現し,その後,心外膜側に及ぶ.この考えに従うと,心内膜側の長軸機能解析は「左室機能障害の早期発見」に有用である1).
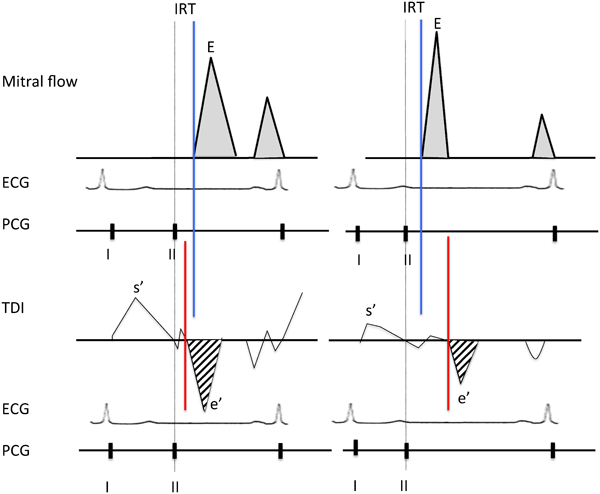
弁輪部は,収縮期に心尖部へ移動し(s′波),拡張期には拡張早期と心房収縮期に2峰性に心基部側へ移動する(e′波およびa′波).a′波とs′波の間には2相性の小さな波形を認め,等容性収縮期(isovolumic contraction time: ICT)に相当する.また,s′波とe′波の間にも2相性の波形を認め,等容性拡張期(isovolumic relaxation time: IRT)にあたる(Fig. 1).
TDIによる心機能分析には以下のような多くの利点がある.i)e′波は前負荷の影響を比較的受けにくい,ii)断層画面が不鮮明な症例でも良好な分析ができる,iii)時間分解能が3~4 msecと極めて良い,iv)左室内径短縮率では得られない長軸方向の心機能を評価できる,v)通常の心エコー装置で解析可能である.一方,欠点としては,i)角度依存性である,ii)心臓全体の動き(translation)や周辺組織の収縮の影響を受ける(tethering),iii)局所壁運動異常がある場合には心室全体の心機能を反映しない,などが挙げられる.
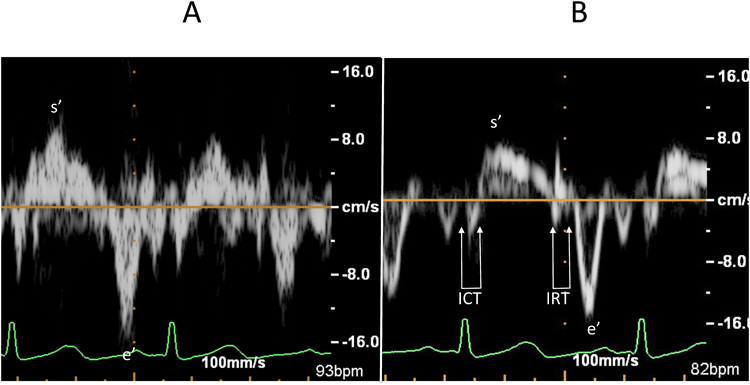
ここで,解析に適した記録を得るためのコツについて触れたい.まず弁輪の運動方向とドプラカーソルはできるだけ平行に設定する.また,良好なドプラ波形を検出できるように,サンプルボリューム幅はやや広めとする(著者は学童で5~6 mmにしている).ドプラゲインは可及的に下げスペクトル包絡線(envelop)が認識できる記録が望ましい.ゲインを上げすぎるとノイズを拾い運動速度を過大評価するばかりでなく,時相解析が困難になるからである.最後に,低速の運動速度を記録するためドプラフィルターは可及的に低く設定する(Fig. 2).
僧帽弁輪収縮期運動速度s′
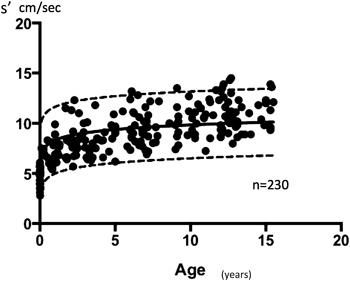
TDIの分析では発育(年齢)を考慮する必要がある(Fig. 3).「s′が年齢と共に増加する」点は,三尖弁輪収縮期運動速度s′でも同様であるが,右室心筋は左室心筋より長軸方向の運動が主体であり,いずれの年齢でも右室s′>左室s′である点は興味深い2, 3).
左室s′波はしばしば2峰性となる(Fig. 1).その成因は不明であるが,Marciniakらは,三尖弁輪から心尖方向へ向かう大きな右室s′波が僧帽弁輪からの左室s′波とぶつかることで左室s′波にdipを形成すると指摘した4).一方,Okiらはs1′波が左室心内膜側の斜走筋(長軸方向の運動に関与)を,s2′波は中層の輪状筋(円周方向の運動に関与)の運動を反映しているとし,長軸機能に関与するs1′波の解析が重要であると報告した5).
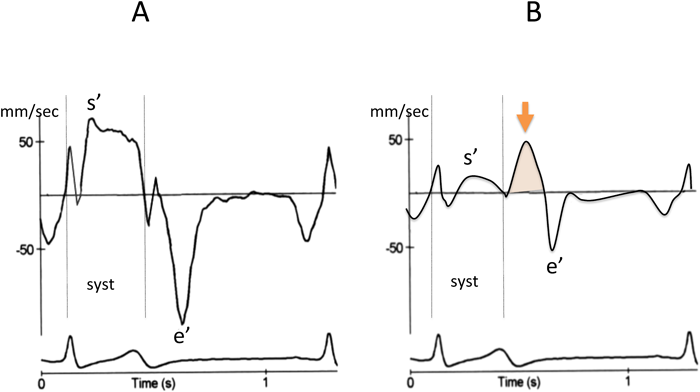
虚血や線維化で局所的に収縮能が低下した心筋では,拡張早期に心筋が短縮する場合がある(Fig. 4).すなわち,周辺の正常心筋が収縮する際には異常心筋は引き延ばされる.その後,正常部位の収縮が終る拡張早期に,延ばされたバネが戻るような受動的な動きとして短縮する.この拡張早期の心筋短縮はpost-systolic shortening(PSS)と言われており,有効な収縮ではない6).このような心筋では収縮期運動速度s′自体は低下している点に注意すべきである.
僧帽弁輪拡張早期運動速度e′
e′も,年齢(体格)に伴い増加する(Fig. 5).乳児期早期の急速な増高は左室拡張能の成熟を示唆している.なお,右室のe′は年齢による変化が少ない7)(Fig. 6).
e′は前負荷の影響を比較的受けにくく,一般に左室拡張能の低下に伴い減高を続ける.一方,僧帽弁口拡張早期血流速度Eは弛緩障害では減高するが,左室コンプライアンスが極度に低下すると増高し急峻となる.そのため,E/e′が左室充満圧の評価に利用されている.小児では,出生直後の新生児ではE/e′が高値となる.出生直後は動脈管のため僧帽弁拡張早期血流速度Eが増高するが,前負荷の影響を受けにくいe′の増高が少ないためである.その後,左室拡張能の成熟に伴いe′が増高するため,E/e′は低下する8)(Fig. 7).
E/e′は左室充満圧を推定するうえで有用とされてきたが,以下の状態では注意が必要である.i)高心拍出状態では,左室充満圧が上昇していても,e′のみならずEも上昇するためE/e′は増加しない9).ii)極度の心機能低下例では高い左房圧が弁輪を押し下げることで高いe′を形成しE/e′は高値とならない10).
e′波の解析では僧帽弁血流E波との時相関係にも注目するとよい.正常では,e′波(左室伸展)の開始時相はE波の開始時相とほぼ同時か若干先行する.しかし,高度の拡張機能低下例では,E波の出現後,大きく遅延してe′波が出現する11)(Fig. 8).
Tei index
ICTは左室最大陽性dP/dtと相関し,収縮能の低下で延長する.またIRTは左室最大陰性dP/dtと相関し,拡張能低下で延長する.駆出時間(ejection time: ET)は1回心拍出量が低下すると短縮する.Tei indexは(ICT+IRT)/ETで算出され,心拍数に依存せず収縮能と拡張能を統合した総合的な心指標であり,心機能障害例では高値となる(Fig. 9).
Tei indexはM-modeやパルスドプラ法(僧帽弁血流と左室流出路血流を用いる)でも測定可能であるが,TDIを用いる方法が最も簡便である.ただし,前2者に比してTDIでの正常値が高値となることを知っておくべきである12).
正常小児では新生児早期はしばしば0.6以上となるが,幼児期以降は年齢によらず平均値0.39程度であり0.6以上を示す例は稀である(Fig. 10).
右室機能と組織ドプラ
右室機能の特徴として以下の4点が挙げられる.i)左室と異なり複雑な形態をしており,血流は「ふいご」状に自由壁と中隔で押し出される,ii)心筋走行は左室のような輪状筋を有さず,内層と外層の2層構造で長軸方向が主体である,iii)心筋コンプライアンスが大で,前負荷に強く拡張障害を生じにくい.一方,後負荷には弱い,iv)外層筋は左室とつながり,心室間相互作用を認める.特にii)は重要であり,TDIによる三尖弁輪収縮期運動速度(s′)が右室機能評価として分析される理由である.成人ではTDIを用いた右室心機能評価が広く認められており,右室s′<10 cm/sec, Tei index>0.55, E/e′>6は「右心機能の異常」と判定される13).また,iv)の観点から,右室機能低下の合併が左心不全患者の予後を規定するとの指摘がある.Damyらは成人の左心不全患者で右室s′<9.5 cm/secは他の右室機能指標に比し予後を予測しえたと報告した14).小児の検討では,術後に右室圧負荷や容量負荷が残存すると経年的に右室s′が低下する15).
僧帽弁輪収縮期移動距離(MAPSE)
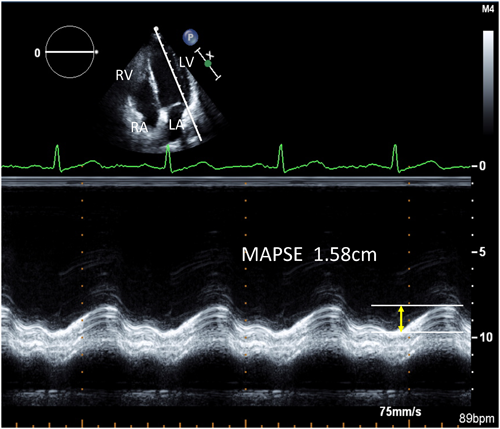
ここまでTDIを用いた長軸機能に関して概説してきたが,M-modeを用いても長軸機能の評価は可能である.すなわち,心尖部四腔断面で外側僧帽弁輪にカーソルを設定し,その移動距離を測定する(Figs. 11, 12).この指標はs′波を時間積分したことになり,最も簡単な左室長軸機能指標と言える.測定に際しては,弁輪運動方向がM-modeのビーム方向に平行となるよう工夫する.
DillerらはFallot四徴症術後413例の検討から,MAPSEが術後突然死や致死的不整脈出現の予測に有用であることを示した16).
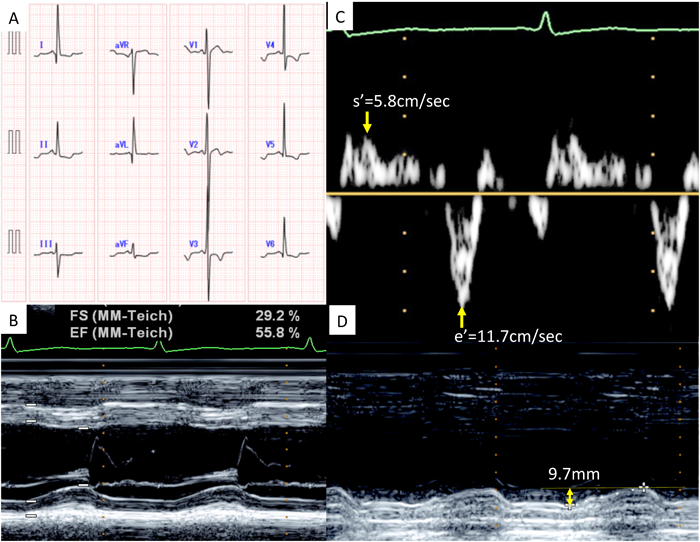
Fig. 13は,学校心電図異常で紹介された左室緻密化障害(15歳男児)の1例である.左室内径短縮率は29%で,軽度低下を認めた.左室長軸方向のTDIではs′とe′共に軽度低下していた.MAPSEは著明に低下しており,心筋障害が強く示唆された.
三尖弁輪収縮期移動距離(TAPSE)
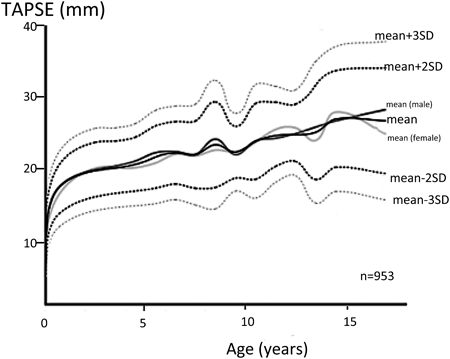
三尖弁輪の収縮期移動距離も心尖部四腔断面からM-mode法で測定可能である.上記のように右室形態は複雑であり,TAPSEは簡便で再現性のよい右室長軸機能指標として提唱されている.正常値はMAPSEと同様に体格(年齢)と共に増加する17)(Fig. 14).Forfiaらは成人の肺動脈性肺高血圧患者で,TAPSE<1.8 cmが予後不良であると報告した18).MoceriらはEisenmenger症候群の心エコー指標を検討し,TAPSE<15 mm,右室の収縮時間/拡張時間>1.5,右房面積>25 cm2,(右房/左房面積比>1.5)の症例が予後不良であることを示した19).Fallot四徴症術後症例でもTAPSEが検討されており20),今後も多くの疾患で他の右心機能指標との対比がなされていくであろう.