冠動脈の解剖学的異常は心臓の働きに直接的な影響をおよぼす可能性があり,突然死の原因となり得ることが知られている.Eckartら1)のmilitary recruit(18~35歳)630万人の調査ではnontraumatic sudden death 126例中39例が冠動脈の異常であったという.また,若年アスリートの死因の19%は冠動脈異常によるとの報告もある2).すなわち健康な若年者の突然死において冠動脈異常の関与の割合が高いことを示唆している3).
冠動脈の形態には多くのバリエーションがあり,どこから異常とするかは意見が分かれる.Angeliniら4)は冠動脈の形態を詳細に検討し分類している.Kayalarら5)は実際の臨床に対応した簡潔な分類を示している(Table 1).発生頻度は検査法や対象者によって異なるが,Yamanaka & Hobbs6)は126,595例の冠動脈造影の検討で冠動脈異常の発生頻度を1.3%と報告しており,文献的にも0.6~1.55%であったという.
Table 1 Classification of coronary artery anomalies| Anomalles of Origin and Course |
| I. Anomalous location of the coronary ostium |
| a. High ostium |
| b. Commissural ostium |
| II. Anomalous orgin of the coronary artery from the opposite sinus with one of 4 courses |
| a. Inter-arterial |
| b. Transseptal |
| c. Retroaortic |
| d. Prepulmonic |
| III. Anomalous origin of the coronary artery from the pulmonary artery |
| Type 1: ALCAPA |
| Type 2: ARCAPA |
| Type 3: Anomalous origin of Cx from PA |
| Tupe 4: ALCAPA and ARCAPA |
| IV. Single coronary artery |
| V. Multiple ostia |
| VI. Anomalous origin of the coronary artery from the noncoronary sinus |
| VII. Duplication of coronary arteries |
| Anomalies of Intrinsic Coronary Arterial Anatomy |
| I. Congenital ostial stenosis |
| II. Coronary artery ectasia or aneurysm |
| III. Myocardial bridging |
| Anomalies of Termination |
| I. Congenital coronary artery fistula |
| II. Extracardiac termination |
| ARCAPA, anomalous origin of right coronary artery from pulmonary artery; ALCAPA, anomalous origin of left coronary artery from pulmonary artery; Cx, circumflex coronary artery; PA, pulmonary artery. (Reproduced from reference 5) |
今回,その危険性が臨床的に特に問題となる3つの疾患,すなわち,①Anomalous origin of coronary artery from the opposite sinus(反対側バルサルバ洞からの冠動脈起始),②Anomalous origin of coronary artery from pulmonary artery(肺動脈からの冠動脈起始),③Coronary arteriovenous fistula(冠動脈瘻),について述べる.
Anomalous origin of coronary artery from the opposite sinus
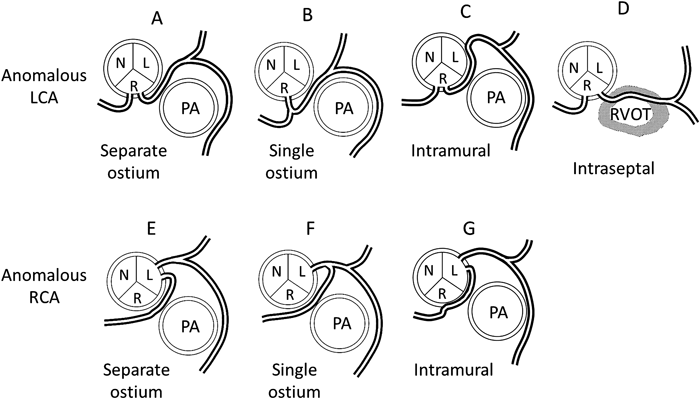
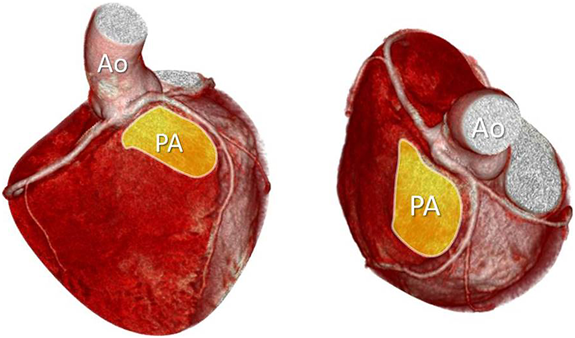
左冠動脈(LCA)が右のバルサルバ洞から起始する場合と右冠動脈(RCA)が左のバルサルバ洞から起始する場合とがある(Fig. 1).また左右冠動脈が別の開口部を持つ場合と単冠動脈として起始する場合がある7).さらに大動脈起始後の走行にはpreaortic course, prepulmonary course, intraseptal courseなど様々なバリエーションがある8).なかでも心筋虚血症状や突然死などの危険性の高いものとして,両大血管間(大動脈-主肺動脈間)の走行9)が挙げられる(Fig. 2).このなかには大動脈壁内を走行するもの(intramural course)がある.
両大血管間走行症例の心筋虚血発生のメカニズムとして,両大血管間からの圧迫10),器質的な狭窄の合併11, 12),さらに大動脈からの起始直後にヘアピン様の急激な屈曲を呈することが虚血の原因となるとの報告もある13).壁内走行を伴う症例では壁内部分の内腔狭窄,入口部のスリット状の狭窄,大動脈からの起始部分の狭窄,などが虚血の原因と考えられる14, 15).
術前診断のうえで臨床症状,あるいは通常の生理検査は必ずしも役に立たないことがあり注意を要する.Bassoら16)のyoung athleteの突然死27例(LMT右バルサルバ洞起始–23例,RCA左バルサルバ洞起始–4例)の検討では,臨床データの残っていた12例中でイベント前に何らかの心症状(exertional syncope/chest pain)を呈していたものが10例あったが,心電図および負荷心電図で陽性を示したものは1例もなかった.すなわち,心疾患を疑わせるような自覚症状を示す症例に対して冠動脈異常を疑った場合には,たとえ心電図で異常を示さなくとも冠動脈のイメージング(心エコー,血管造影,CT,MRI)を行うべきである17).
手術適応として,ACC/AHAガイドライン18)では以下のいずれかがあれば外科的冠血管再建術を行う(クラス1)としている.
- a. Ao–MPA間をLMTが走行する場合(エビデンスレベルB)
- b. 冠動脈圧迫による冠虚血が確認された場合(Ao–MPA間を冠動脈が走行する場合や壁内走行の場合)(エビデンスレベルB)
- c. RCAがAo–MPA間を走行する症例で虚血が確認された場合(エビデンスレベルB)
また,Mayo clinicから報告された治療方針19)は以下のようである.
- a. Ao–MPA間をLMTが走行する場合は全て手術
- b. Ao–MPA間をRCAが走行する場合symptomaticであれば手術
- c. ストレステスト陽性の場合,active lifestyleを望む患者には手術
- d. Ao–MPA間をnondominant RCAが走行する場合にasymptomaticの患者は保存的に対処
さて,臨床の場で頭を悩ますのは,無症状の本疾患患者に遭遇した場合どのような対処が望ましいかという点である.症状の有無を問わずLMT右バルサルバ洞起始症例の発生頻度についてYamanaka & Hobbs6)の報告では126,595例中22例(0.017%)となっており,まれな疾患であることがわかる.しかもこれは心臓カテーテルを受けた患者のみのデータであるため有症状患者が含まれているであろうこと,また平均年齢が53歳と比較的高く,突然死の患者はすでに除外されている可能性があることから,実際の臨床の場で無症状の本疾患患者に遭遇する可能性は極めて低いことが予測される.このような状況の中で担当医師自身が本疾患の危険性を熟知し,丁寧に根気よく説明して手術を納得してもらう必要がある.
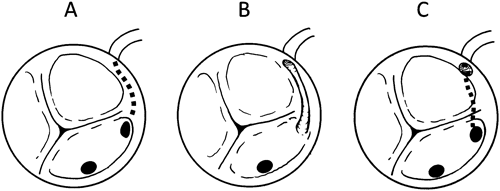
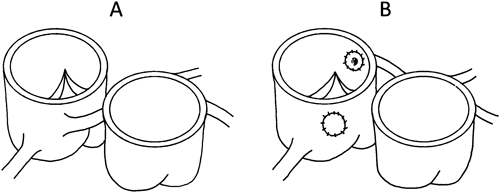
手術法については解剖学的特徴に従った術式が選択される.unroofing/fenestrationは壁内走行に対して行われる方法である.unroofingは壁内走行部全体を大動脈内腔に開放する方法である(Fig. 3B).壁内走行部分が大動脈弁交連頂点より下方を走行する場合には弁機能を障害する危険があるため,交連部を避けて新たに大きな冠動脈開口部を作成するfenestration(Fig. 3C)が行われる19, 20).reimplantationは左右冠動脈口が別個に開口している場合,冠動脈を周囲の壁ごとボタン上に切り出して両大血管間を通らないような位置に移植する(Fig. 4).coronary artery bypass grafting(CABG)も外科治療として行われるが,通常の状態では狭窄も虚血も認めない症例の場合,果たしてバイパスが長期間開存しているかどうか不安な部分もある.逆に冠虚血の著しい緊急症例に対してCABGは良い適応と考えられる12).主に若年者が対象となるので長期開存が期待できる動脈グラフトの使用が望ましい.translocation of the pulmonary trunkは両大血管に挟まれた部分の圧迫を解除する目的で,主肺動脈を切断し左方に移動させるleftward mobilization21),および右肺動脈を分岐部付近で切断し大動脈の前方に移動させるanterior mobilization7)が報告されている.しかし症例数も少なく,はたしてどのくらいの効果が期待できるのかまだ不明である.coronary stentingはカテーテルによる緊急治療で,心肺蘇生を行いながら壁内走行のLMTにstentingを行ったが,のちに狭窄のためCABGを行ったとの報告がある22).
まとまった数の手術成績の報告は少ない.Daviesら19)は冠動脈が反対のValsalva洞から起始し両大血管間走行する患者36例(13~82歳)の手術を報告している.34例に壁内走行を認め,うち22例にunroofingが,また残りの14例にはCABGが行われた.結果は,手術死亡・遠隔死亡なく,CABGの1例で胸痛の再発を認めたのみであり,unroofingの成績は極めて良好であった.
Anomalous origin of coronary artery from pulmonary artery
左冠動脈が肺動脈から起始する疾患(Anomalous origin of left coronary artery from pulmonary artery: ALCAPA)は,従来よりBland–White–Garland(BWG)症候群と呼ばれていた.左冠動脈が肺動脈から起始する場所は後洞あるいは左洞が多く,まれに右洞のこともある23).極めてまれであるが肺動脈末梢からの起始も報告されている24).自然歴では90%の患者が乳児期に死亡し,RCAからLCAへの側副血行の発達の良い症例だけが成人に達するが(Adult type)そのような症例は極めてまれである.通常の症例(Infant type)は早期から心筋虚血が強く心筋梗塞からischemic cardiomyopathy(ICM)を呈する25, 26).突然死も知られており27),また左室拡大による弁輪拡大および乳頭筋機能不全から僧帽弁閉鎖不全(MR)を生じやすく,こちらが主要な徴候で発見されることも多い.
診断のうえでは,ICMやMRを呈する乳児を見た時,本疾患をまず疑うことが重要である.心エコーによる肺動脈内のシャント血流,前下行枝の逆行性血流,右冠動脈の拡張などの所見から確定診断に至る.手術のためにはLCA起始部の正確な位置が必要なので造影CTが勧められる.
手術では,以前はLMTの結紮も行われたが,新たな側副路の発達により再び虚血を生じるとの報告があり,two-artery coronary systemの確立が必須である.これまでTakeuchi法28)(肺動脈内のトンネルにより大動脈との交通を作成する)など,多くの手術法の報告がなされているが,術式選択にはLCA開口の位置が重要となる.すなわち開口から大動脈までの距離が近い場合には,直接吻合法が可能である29, 30).しかし開口から大動脈までの距離が遠い場合,特に右洞起始の場合などにはこれらの術式は困難なことが多く,何らかの冠動脈の延長が必要となる.肺動脈壁を大きく取ってチューブ状にする31),肺動脈壁のフラップを使ってラセン状の延長部分を作成するspiral cuff technique32)(Fig. 5),大動脈壁フラップと肺動脈壁フラップの両者を吻合するdouble flap technique33, 34)(Fig. 6),などの工夫が報告されている.
手術成績は比較的良好とされ35),Hoashiら23)によると手術死亡は0~16%であるが,morbidityおよび再手術率の高さが目立つ.また,以前より本疾患に伴うischemic MRは遠隔期に改善するので弁形成を加える必要はないとの意見が多かったが36, 37),Isomatsuら38)はKay-Reedタイプの比較的単純な弁形成を行うことで遠隔期の良好なMRの改善を得られたとして弁形成を加えるべきと述べている.
右冠動脈が肺動脈から起始する場合(Anomalous origin of right coronary artery from pulmonary artery: ARCAPA)はALCAPAに比して全般に症状は軽く,心不全や心筋虚血症状を呈することはまれである.突然死はまれにあるとされている39, 40).手術の危険は低いため,診断された症例は全て手術適応と考えられる.RCAを周囲の肺動脈壁とともに上行大動脈に移植する41).
Coronary arteriovenous fistula
冠動脈瘻(CAVF)は,冠動脈が近接する心血管腔に直接開口する異常で,Levinら13)の報告ではRCA(52%),LCA(43%),RCA & LCA(5%)42)の順に多く,流入する部位は右心系に多く,Loweら43)によるとRV(40%),RA(25%),PA(20%),CS(7%),SVC(1%)の順であったという.
小さな交通は無症状のことが多く,検査で偶然発見される場合が多い44).大きなCAVFは冠血流のスチール,シャント量,が問題となり,狭心痛,労作性呼吸困難,易疲労感などを呈する.瘤の形成が報告されているが破裂に至る例はまれとされる.冠静脈洞に開口するCAVFでは心筋のうっ血により心不全を呈しやすいとの報告がある45).感染性心内膜炎の原因の一つに数えられる.他覚的には連続性雑音の聴取,胸写上の心拡大などが挙げられる.発生頻度の詳細は不明であるが,小児では心エコーを受けた患者の0.06%46)に,また先天性心疾患患者の0.3%程度47)にみられるとの報告がある.一方,冠動脈造影を受けた成人では0.13~0.22%にみられるという6, 48–50).CAVFは基本的に出生時から存在するものであり,検査法の違いもあって小児と成人におけるこの頻度の差が果たして実際を表しているかは不明である.しかし,中には経過観察中にCAVFの径やシャント量が増大を示すものや合併症を生じてくるものなどがあることから,臨床的に有意なCAVFの発生は年齢とともに増加すると思われる.
診断は,心雑音などの理学所見や臨床症状から疑い,心エコー,冠動脈造影,CTアンジオなどで確定する.なかでも冠動脈造影は中心的な検査であり,CABGが必要かどうかの判定や,治療としての塞栓術の際にも用いられる.
ACC/AHAガイドライン18)によるとCAVFの手術適応は以下のものが挙げられている(クラス1).
- a. 大きなCAVFは症状によらずカテーテルか手術により閉鎖する(エビデンスレベルC).
- b. 小~中等大のCAVFは,心筋虚血,不整脈,心室機能不全,心室拡大,心内膜炎を認める場合に閉鎖(エビデンスレベルC).
手術適応は主にCAVFの大きさと臨床症状によって決められ,年齢は必ずしも関係ないが,若年者と高齢者での手術成績の違いから早期の手術を勧める報告もある50).
治療にはカテーテル治療と外科治療がある.カテーテル治療はCAVFをコイルやその他のデバイスなどで閉鎖するもので,重要な冠血流を遮断する危険がない,コイルが逸脱しにくい瘻の形状,など限られた症例が対象になり,充分経験のある施設で行うべきとされている.外科治療のうち,到達しやすい場所にあって冠動脈の末端部分や重要性の低い分枝に生じたものでは人工心肺を用いずに閉鎖が行える場合がある.人工心肺の使用が勧められるのは,CAVFが拡張・蛇行していてカテーテル閉鎖が行いにくい,心拍動下で到達困難な部位にある,瘻内腔からの閉鎖が必要,CABG併施が必要,などの場合が挙げられる.
手術成績はカテーテル治療でも外科手術でも一般に良好といわれている44).しかし手術後の虚血性の心電図変化,心筋梗塞,不整脈,脳梗塞,CAVFの再発51),などの合併症の発生が報告されている52).